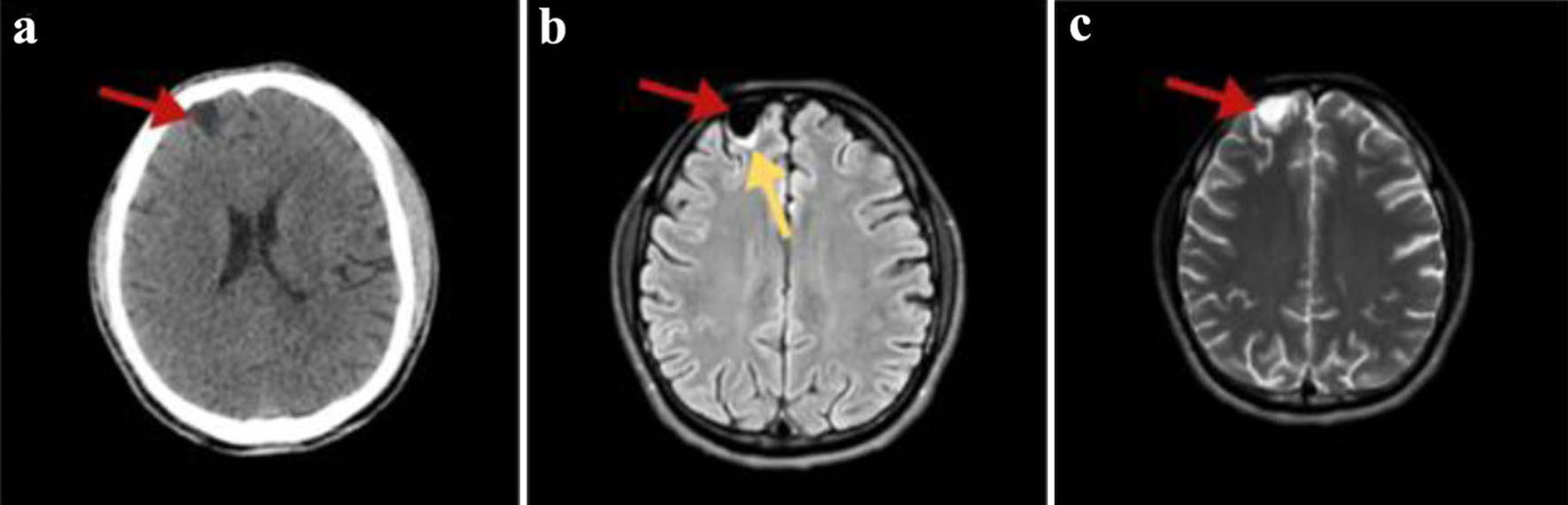
Figure 1. (a) Non-enhanced axial brain computed tomography showing a hypodense right frontal cystic lesion (red arrow). (b) FLAIR MRI axial slices depicting a hypointense homogenous frontal cystic lesion (red arrow) with surrounding gliotic changes (yellow arrow). (c) T2-weighted brain MRI image in the transverse plane presenting the lesion having a non-homogenous pattern (red arrow). In all MRI images, the cyst has similar signal and intensity to those of CSF. MRI: magnetic resonance imaging; FLAIR: fluid-attenuated inversion recovery; CSF: cerebrospinal fluid.
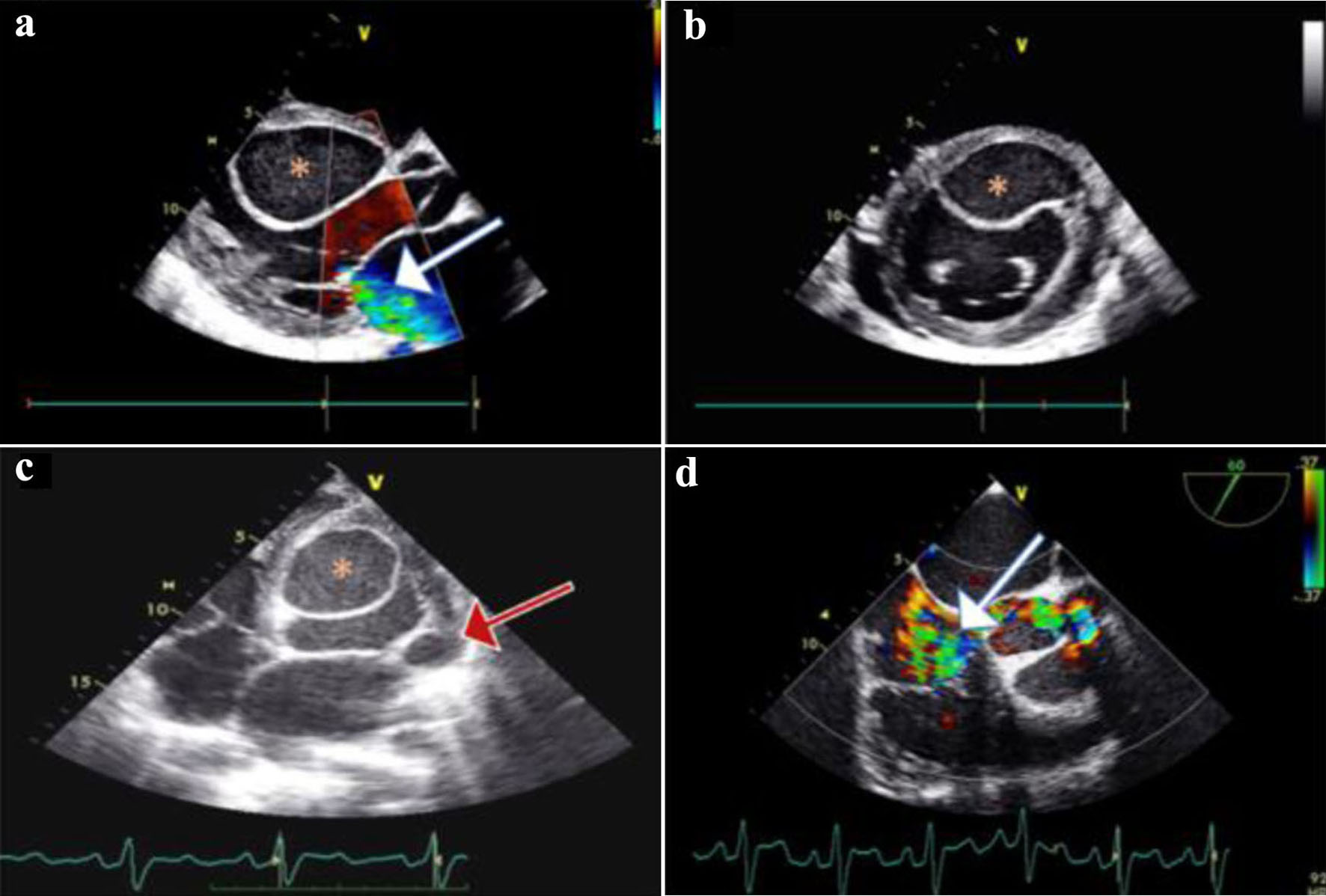
Figure 2. (a) Two-dimensional transthoracic echocardiography (TTE) of parasternal long-axis, showing mild to moderate mitral regurgitation (MR) (white arrow); a large cyst (asterisk) is noticed on the interventricular septum (IVS) protruding in the left ventricle (LV). (b) TTE of parasternal short-axis view showing the IVS cyst protruding in the LV cavity; a small pericardial effusion is also inspected. (c) Transesophageal echocardiogram (TEE) of four-chamber view showing the IVS cyst, and a smaller cyst (red arrow) on the lateral annulus of the mitral valve. (d) TEE mid-esophageal inflow - outflow 60° view showing severe tricuspid regurgitation (TR) (white arrow).
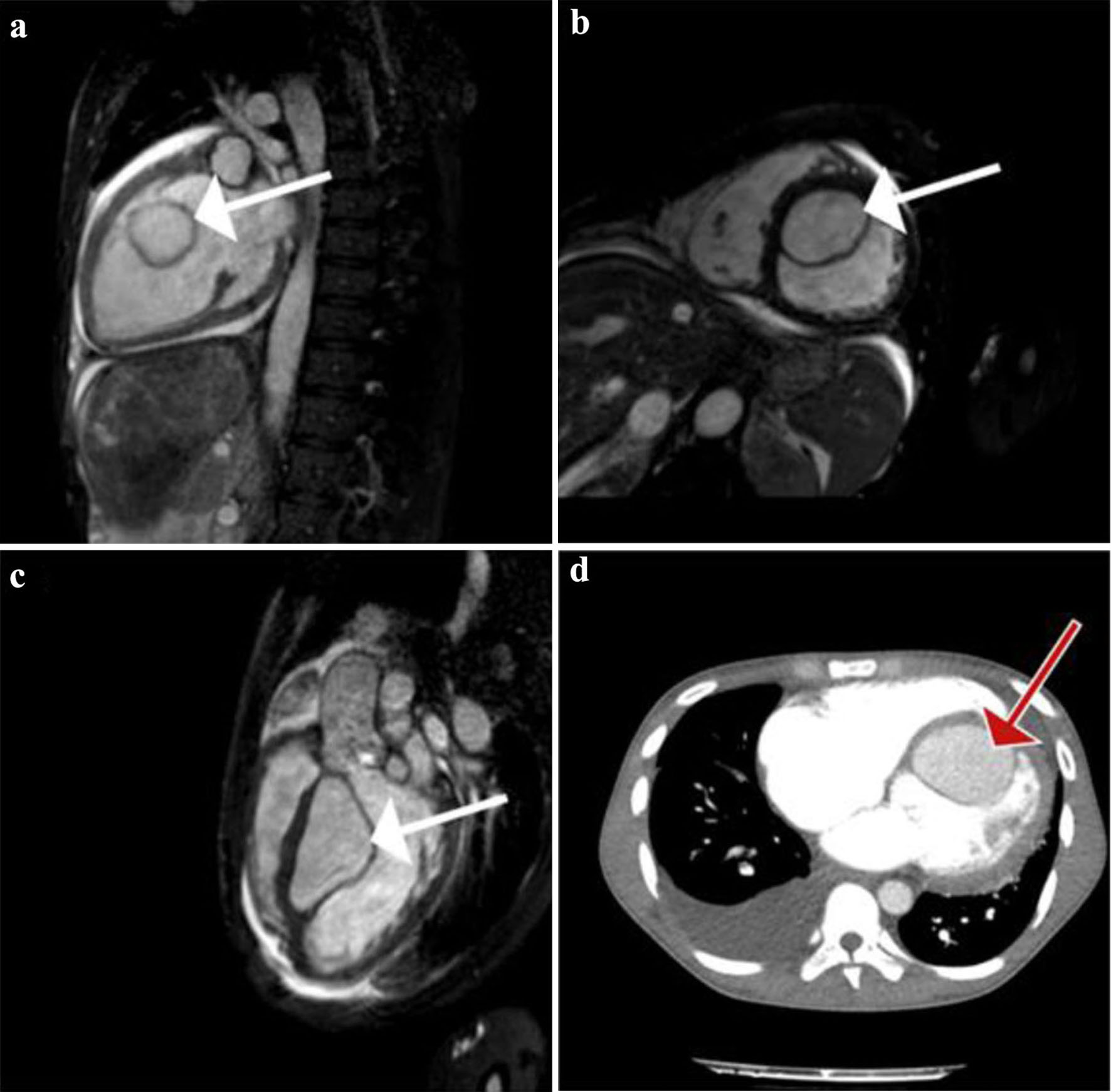
Figure 3. (a) Gadolinium-enhanced vertical long-axis cardiovascular magnetic resonance (CMR) view (or pseudo two-chamber view) clearly showing a large left ventricular (LV) cyst (white arrow). Homogenous enhancement of the cyst and LV’s content implicate the existence of a communication between the two. (b) True short-axis CMR view, where the cyst (white arrow) is seen attached to the interventricular septum (IVS). Simultaneously we see the dilated right ventricular (RV) cavity. (c) Sagittal left ventricular outflow tract obstruction (LVOT) CMR view showing again the intraventricular cyst (white arrow) attached to the IVS. (d) Transverse contrast-enhanced computed tomography (CT) pulmonary angiogram, depicting a large right pleural effusion and the large LV cyst (red arrow). No signs of pulmonary embolism were seen.