
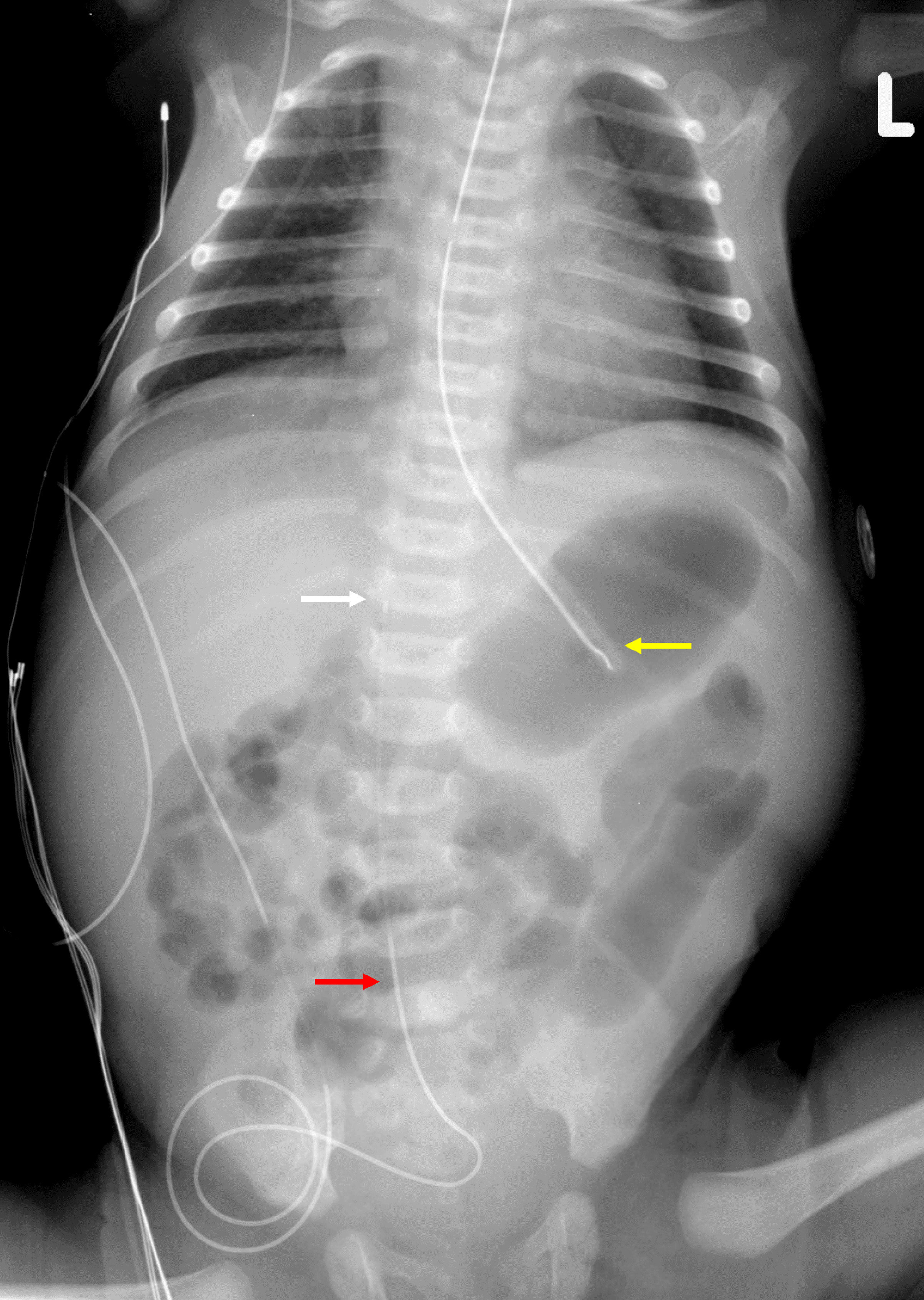
Figure 1. Preoperative radiograph showing the presence of the fetus-in-fetu with calcified bony structures.
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://www.journalmc.org |
Case Report
Volume 14, Number 12, December 2023, pages 393-399
Anesthetic Care During Exploratory Laparotomy and Excision of a Fetus-in-Fetu With a Combined General-Regional Anesthetic Technique Using a Caudal Epidural Catheter
Figures
Table
| Reference | Patient demographics | Anesthetic technique and outcome |
|---|---|---|
| FIF: fetus-in-fetu; US: ultrasound; CT: computed tomography; CDH: congenital diaphragmatic hernia; EXIT: Ex utero intrapartum treatment; MRI: magnetic resonance imaging. | ||
| Traisrisilp et al, 2018 [13] | 1,950-g female infant, FIF excision performed at 2 months of age | Intracranial FIF with mass (9 × 8 × 7 cm) that occupied most of the intracranial space. There was little normal brain tissue thereby resulting in a poor preoperative prognosis. Under general anesthesia, a frontoparietal craniotomy was performed. The neonate had a cardiac arrest intraoperatively and expired. |
| Afshar et al, 1982 [14] | FIF excision performed at 7 weeks of age in a female infant | General anesthesia. A discrete mass with small hairs on its surface was excised from the ventricle of the brain. Uncomplicated postoperative courses. The patient was discharged home 3 weeks after removal of the mass. |
| Runggaldier et al, 2023 [15] | 2,945-g male neonate, FIF excision performed on day of life 2 | Intra-oral location with a stalked feti-form mass (12 × 8 × 5 cm) protruding from the mouth (12 × 8 × 5 cm). Postnatal MRI demonstrated the attachment of the mass to the soft palate with extension to the masseter muscle and the right parotid gland. Limited information on exact anesthetic technique. Postoperative breathing, swallowing and voice production were normal, and the patient was discharged on postoperative day 15. |
| Yu et al, 2018 [16] | 4.1 kg neonate, FIF excision performed on day of life 8 | General anesthesia. Perinatal US showed a complex mass (14.4 × 12.1 × 10.5 cm) with both cystic and solid components arising from the right side of the face and neck. During an EXIT procedure, the trachea was successfully intubated using a rigid bronchoscope. Patient was discharged home on day of life 45. |
| Woodard et al, 2006 [17] | 2,700-g female neonate, FIF excision performed on day of life 2 | General anesthesia. Perinatal US showed a mass (7.3 × 5.4 × 6.0 cm), which was comprised of cystic, solid, and vascular components. It arose from left neck. The EXIT procedure was planned, and she was successfully intubated using direct laryngoscopy. Perioperatively, the baby failed extubation and required a tracheostomy. |
| Derniaux et al, 2010 [18] | 2,910-g neonate, FIF/teratoma excision performed on day 2 of life | General anesthesia. A large perineal mass (5 × 3. 5 × 3 cm) was present arising from the external genitalia. Uncomplicated postoperative course. |
| Gangopadhyay et al, 2010 [19] | FIF excision performed at 10 weeks of age in a male infant | General anesthesia. A well-encapsulated cystic retroperitoneal mass (20 × 8 × 5 cm) was displacing the spleen, transverse colon, and pancreas was excised completely. Uncomplicated postoperative course. |
| Karaman et al, 2008 [20] | Case series of two patients, weight not specified for one and 3,600 g for the second patient; FIF excision performed at 10 and 28 days of age respectively | General anesthesia for both cases. Abdominal FIF (10 × 15 cm) in one patient and sacral FIF in the other. The mass was totally removed, including its capsule for both cases. Coccyx removed in second patient. Uncomplicated postoperative courses. Histopathology for both cases confirmed the diagnosis of FIF. |
| Coolen et al, 2007 [21] | 3,480-g male neonate, FIF excision performed on day 3 of life | General anesthesia. Cystic mass (7 × 4.5 × 4.8 cm) containing solid components (bowel, a thorax with lungs, vertebrae, and a spinal canal) was dissected and removed. Pathological findings were consistent with FIF. No follow-up information provided. |
| Gerber et al, 2008 [22] | 2,665-g neonate, FIF excision performed on day 2 of life | General anesthesia. Intra-abdominal masses consisted of 11 fetoid elements with the presence of a mature teratoma. Although the procedure was tolerated well, the patient died of multisystem organ failure on day of life 34. |
| Santos et al, 2008 [23] | FIF excision performed during two sessions (day of life 9, and 8 months of age) | General anesthesia. There was a retroperitoneal mass extending from the kidneys to the pelvis, sacrum, and coccyx with solid, cystic, and fatty components. |
| Joshi et al, 2009 [24] | FIF excision performed at 6 months of age | General anesthesia. Intra-abdominal mass (15 × 10 cm). US revealed a retroperitoneal mass with calcifications. CT imaging showed an encapsulated mass with fat densities and rudimentary limbs. Complete tumor excision. Histopathology confirmed FIF. |
| Sharma et al, 2012 [25] | Female infant, FIF excision performed at 2 months of age | General anesthesia. Mass in right upper abdomen noted since birth. Firm mass (10 × 12 cm) palpated in the right hypochondrium. US and CT abdomen revealed a mass with cystic and solid calcified components in the retroperitoneum. The mass was completely excised. Histopathological examination confirmed FIF. |
| Khatavkar et al, 2023 [26] | 9-kg infant, FIF excision performed at 18 months of age | Painless abdominal mass since birth as well as constipation, difficult urination for last 3 months. Abdominal CT and US confirmed the diagnosis. Anesthesia included a combined general-regional technique using epidural anesthesia. The epidural catheter was placed at L1 - L2 with an infusion of 0.2% ropivacaine at 2 mL/h. Epidural infusion with 0.1% ropivacaine was continued postoperatively. |
| Agavelyan et al, 2016 [27] | 2,900-g neonate, FIF excision performed immediately after birth | FIF in the epigastrium, omphalocele, and CDH. Anesthesia with a combined general-regional technique using epidural anesthesia. The epidural catheter was placed at L1 - L2 with the catheter tip threaded to T9 - T10. The child died of multisystem organ failure at 25 days of life. |