Figures
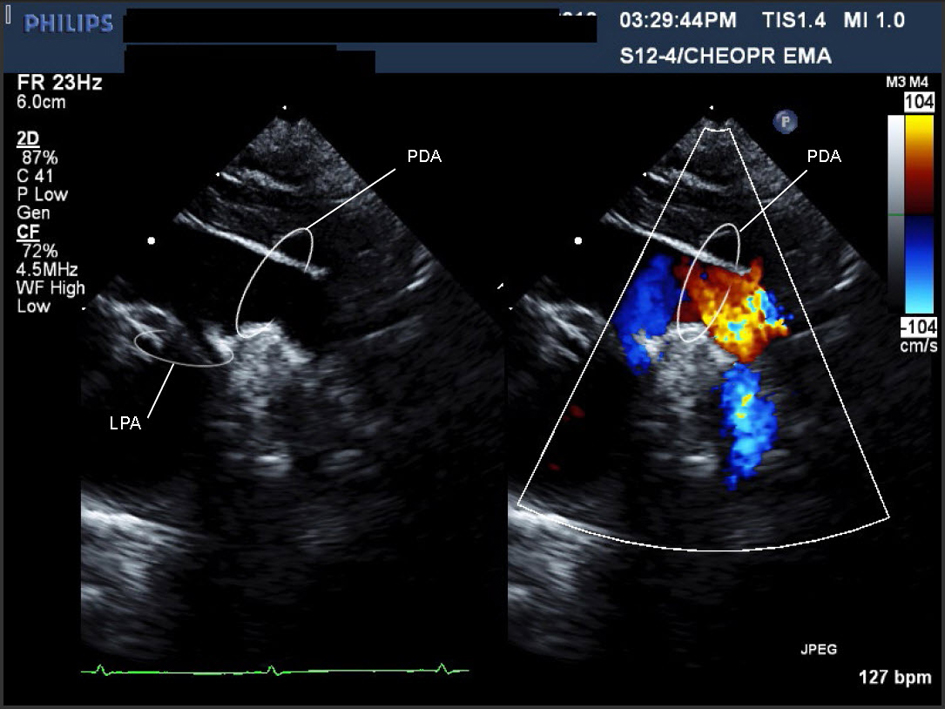
Figure 1. Movie 1. A large PDA (with left to right shunt) was seen measuring 0.72 cm in diameter, compared to a descending aorta diameter of 0.69 cm. Suspected to be on the right side as there was a RAA.
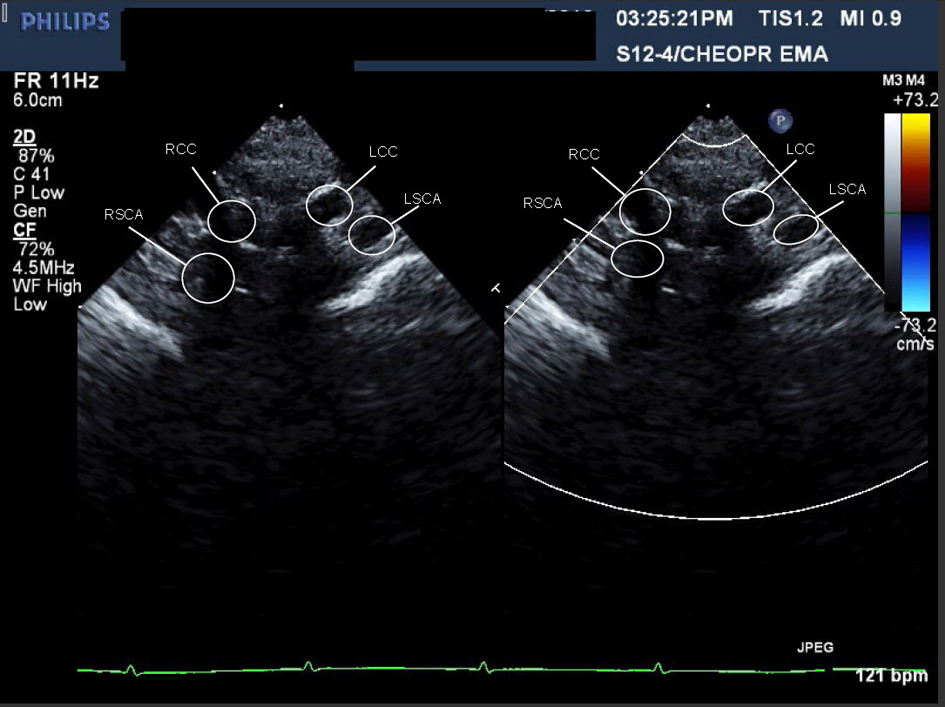
Figure 2. Movie 2. Echocardiographic sweep showing a suspected double aortic arch.
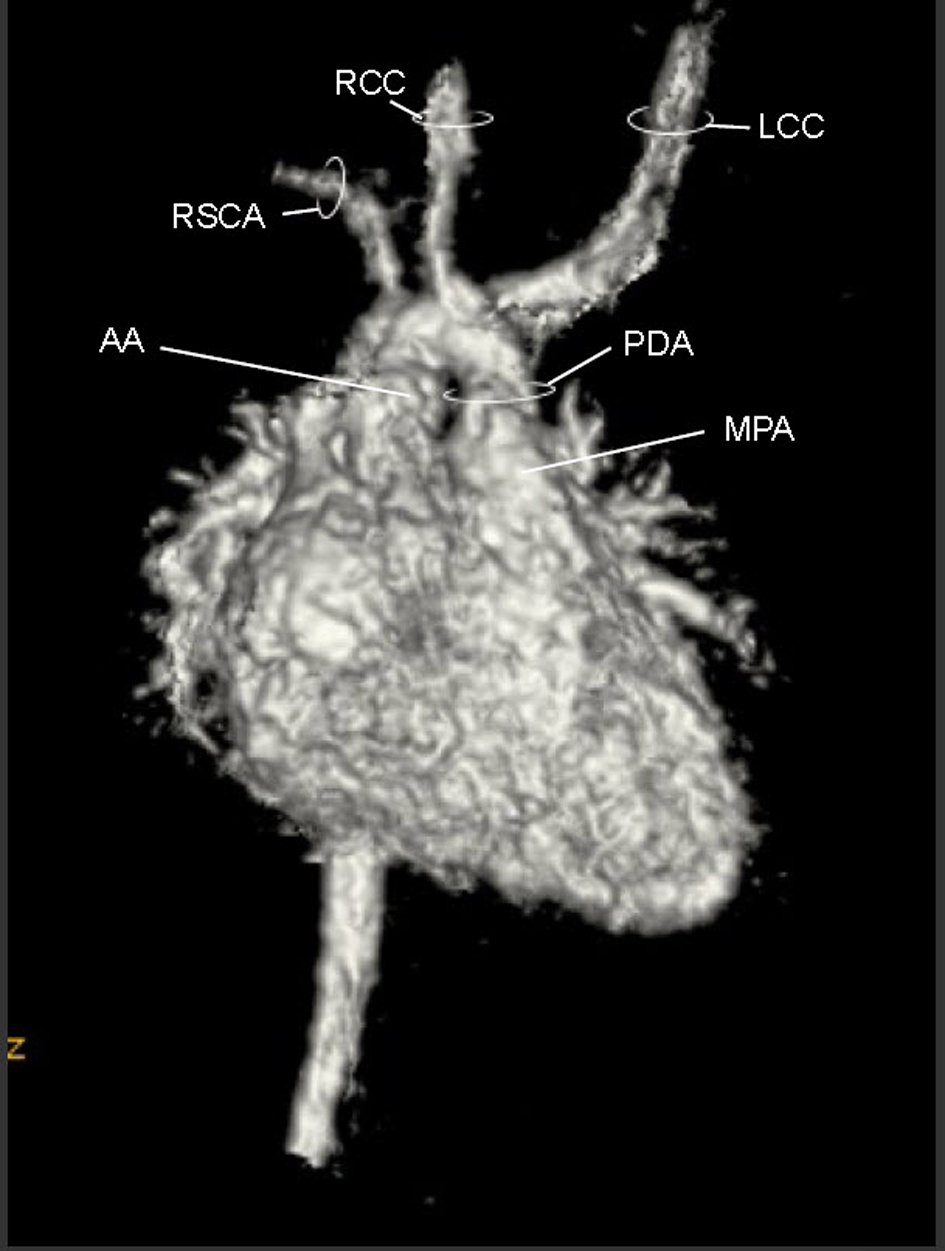
Figure 3. Movie 3. 3D MRI angiogram reconstruction. The study was performed without general anesthetic knowing that some respiratory artifact would be acceptable. The first branch was a suspected BCT giving rise to the RCCA, LCCA, and LSCA, the second branch was the RSCA.
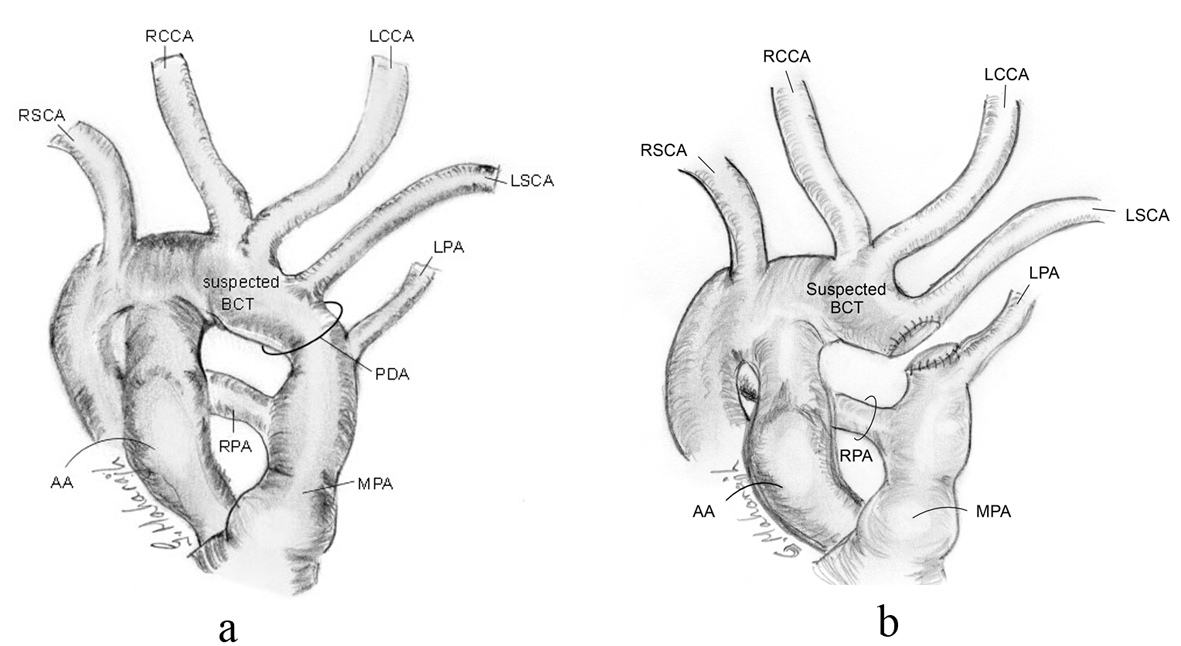
Figure 4. Schematic of intra-operative anatomy showing shortness in length of PDA and relationship of proximity of LPA and LSCA, pre-transection (a), and post-transection (b).
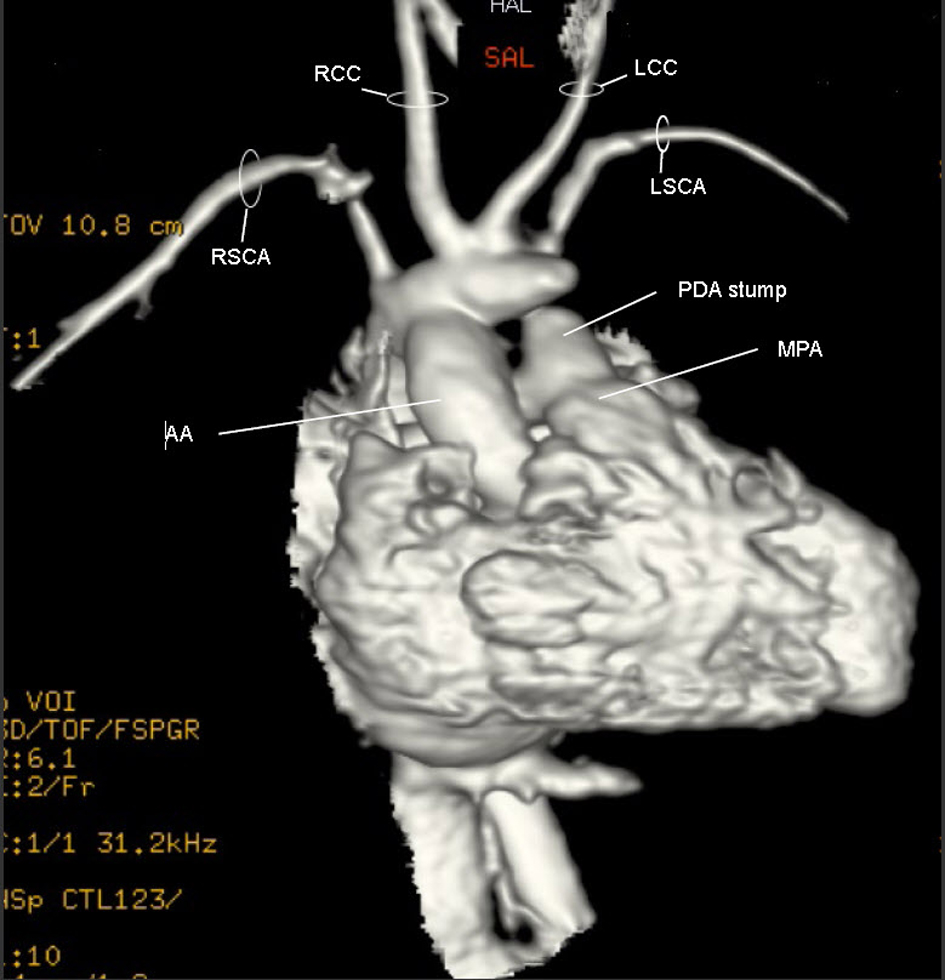
Figure 5. Movie 4. 3D MRI post-op: The suspected BCT was oriented anteriorly such that blood from the ascending aorta took a U-turn to perfuse it. Off the suspected BCT, the RCCA, LCCA and LSCA arose individually and the trunk’s distal end was patched.
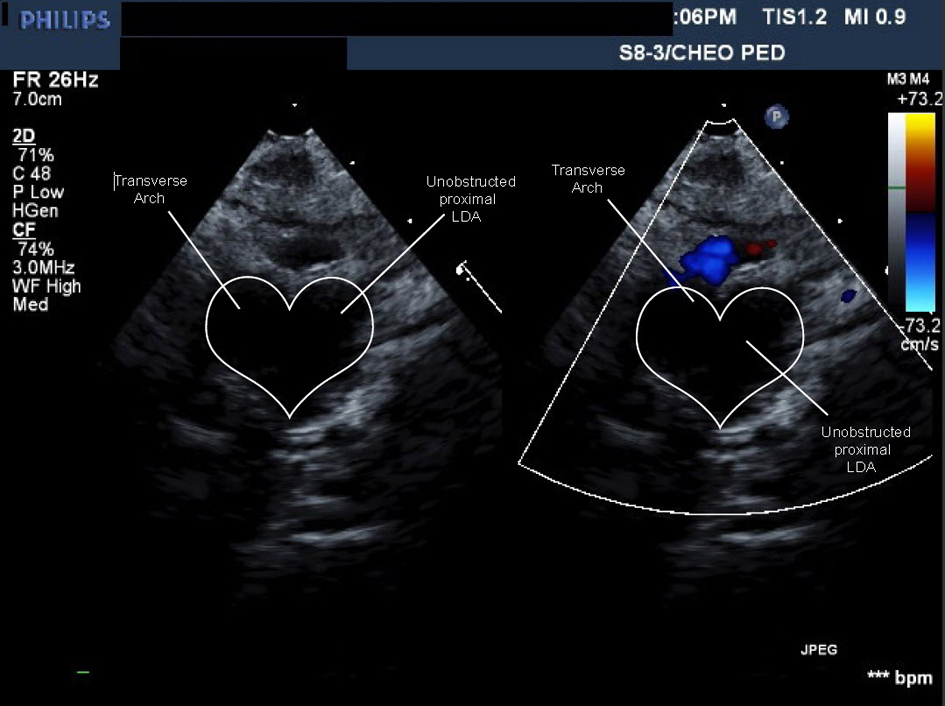
Figure 6. Movie 5. Echo study: forward flow from ascending aorta into large caliber persistent proximal left dorsal aorta then into head and neck vessels without obstruction or flow acceleration.
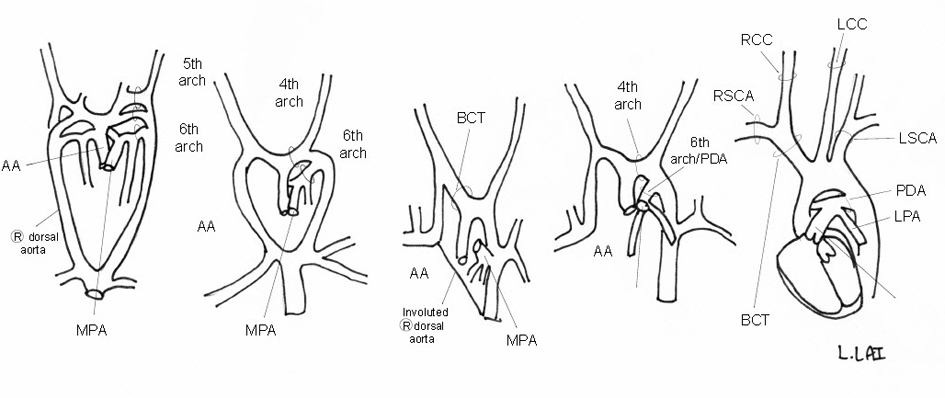
Figure 7. Schematic of embryologic development of a normal LAA.
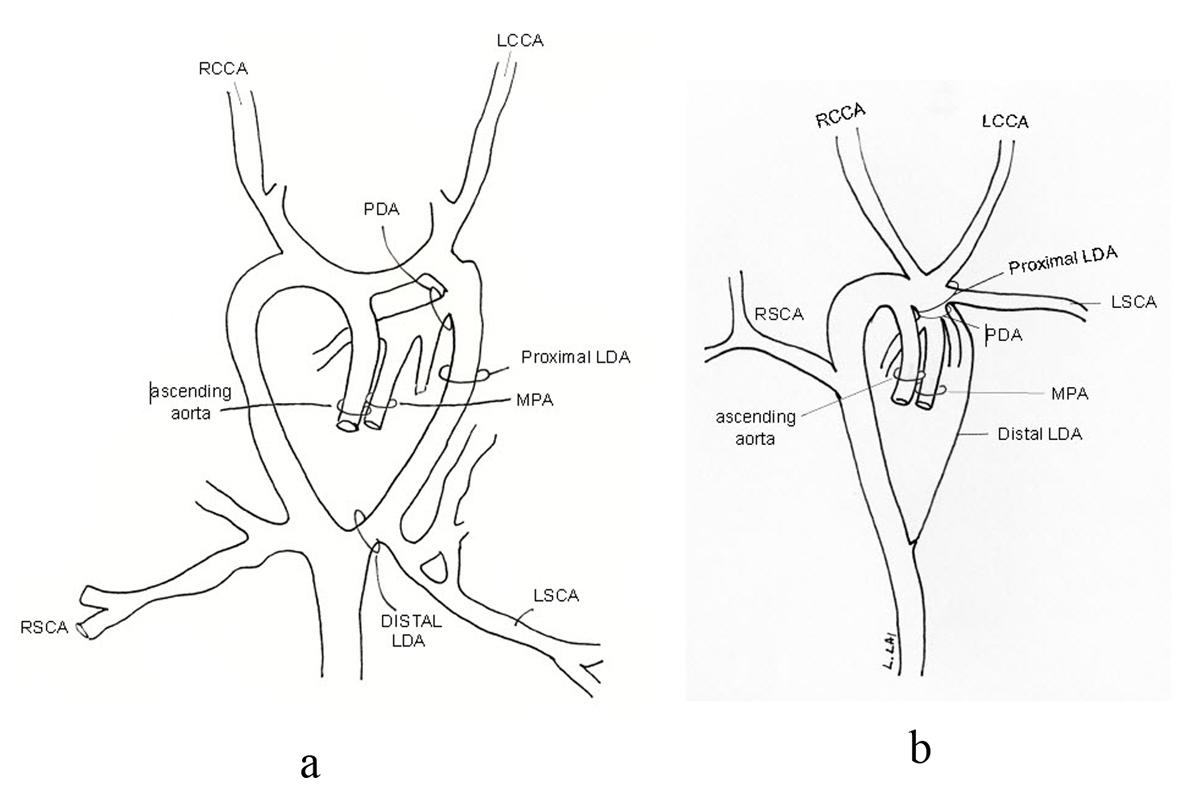
Figure 8. The suspected BCT is actually a large segment of a persistent proximal left dorsal aorta (LDA) (a) making this an incomplete double aortic arch with involution of the distal portion of the left dorsal aorta (b).