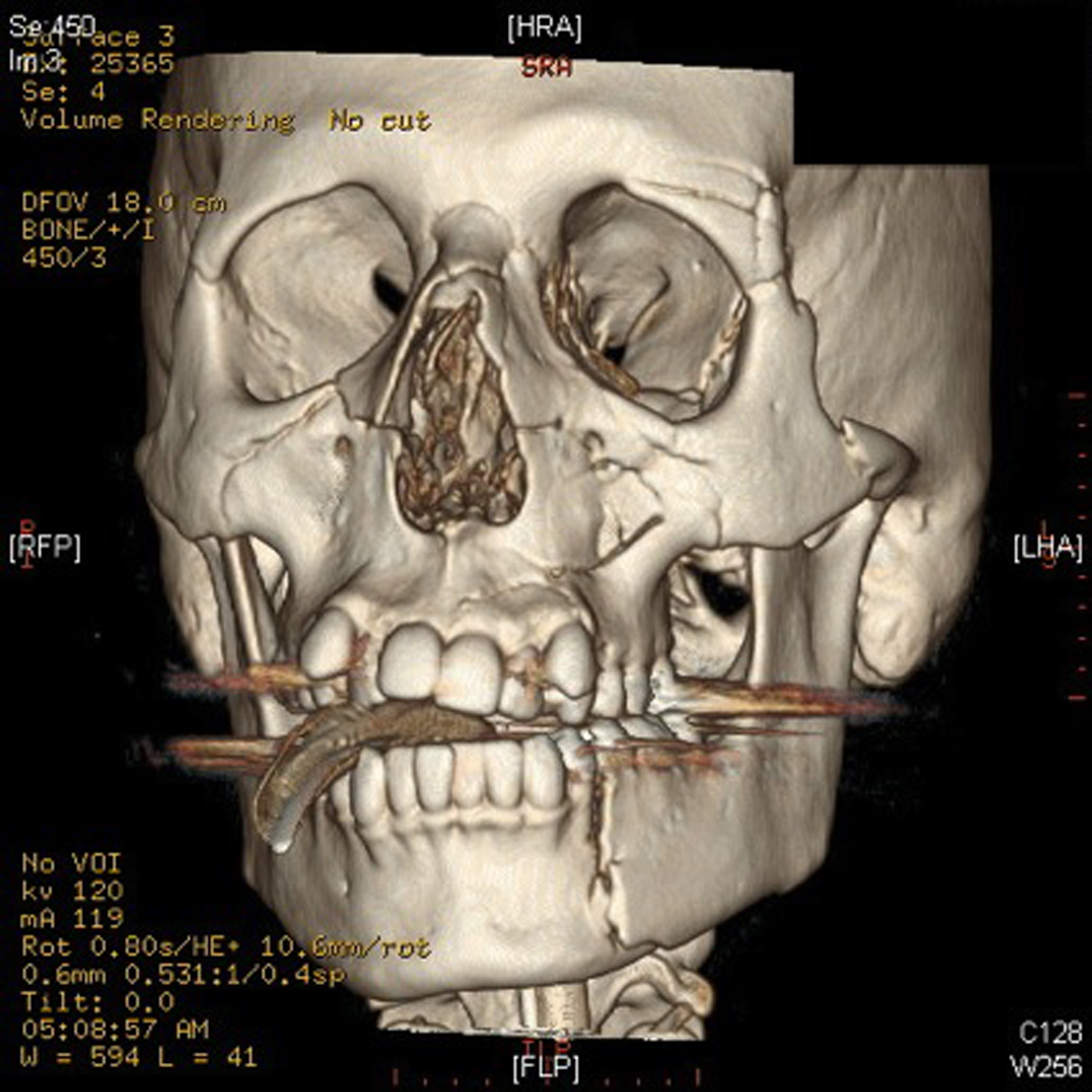
Figure 1. Depicted above is a CT reconstruction of the patient’s facial injuries. These include fractures of the bilateral medial and lateral pterygoid plates, bilateral nasal bones, and left zygoma. Comminuted fractures of the medial and lateral walls of both maxillary sinuses are visualized. There are fractures of the medial and lateral walls of the left orbit, which is comminuted in the lateral wall. There are also bilateral orbital floor fractures, which involve both orbital rims and infra-orbital foramina. There are also several fracture lines extending from the left maxillary sinus into the left maxilla. There is also a fracture through the left mandibular body.