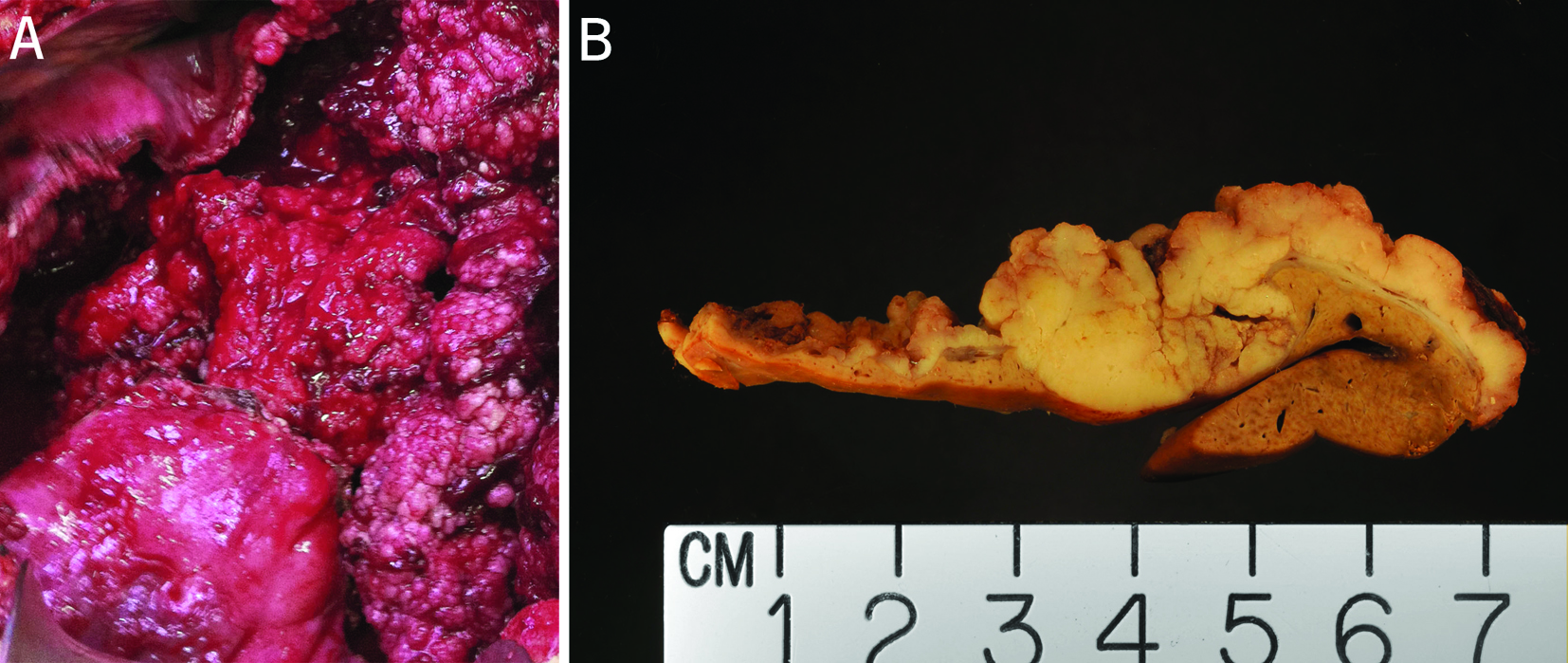
Figure 1. (A) Intraoperative view of the largest cyst. The largest cyst was superficially located and the inner surface of the cyst was irregular with papillae and protuberance of difference sizes and thickness. (B) Cut surface of a portion of the resected cystic lesion from the left lobe of the liver. This cut surface was from the solid area of the cystic lesion. The adjacent cystic wall was irregular with papillation. The tumor was circumscribed, and encapsulated for most part. The adjacent liver did not show evidence of cirrhosis.
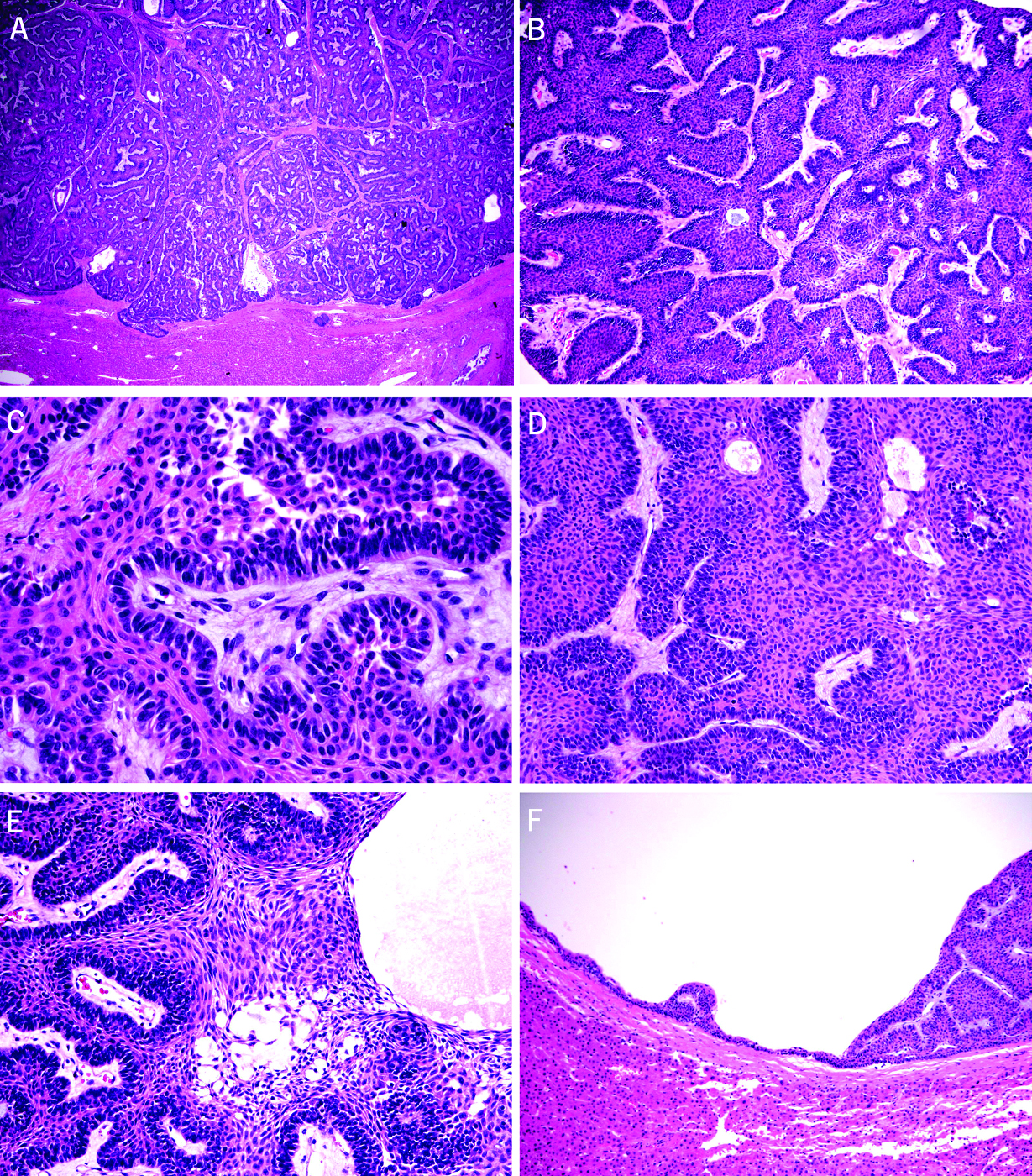
Figure 2. Microscopic features of the resected cystic liver tumors (A-F). (A) Complex architecture of interlocking islands composed of epithelial cells (H&E stain, 20X). (B) Interlocking islands consisted of peripheral palisading of basaloid cells (H&E stain, 40X). (C) Focal reverse polarity noted in basaloid cells (H&E stain, 100X). (D) Obvious squamous differentiation of the centrally located cells with relatively uniform cells containing slightly pleomorphic nuclei, small nucleoli, and moderately abundant eosinophilic cytoplasm (H&E stain, 100X). (E) Mild cystic degeneration and myxoid changes noted focally in the central portion of the islands, resembling the “stellate reticulum” of the dental enamel origin (H&E stain, 200X). (F) A few small cysts lined with an epithelial lining with gradual transition from flat epithelium, early papillation, complex papillation, and solid protuberance noted adjacently to the largest cyst (H&E stain, 20X).
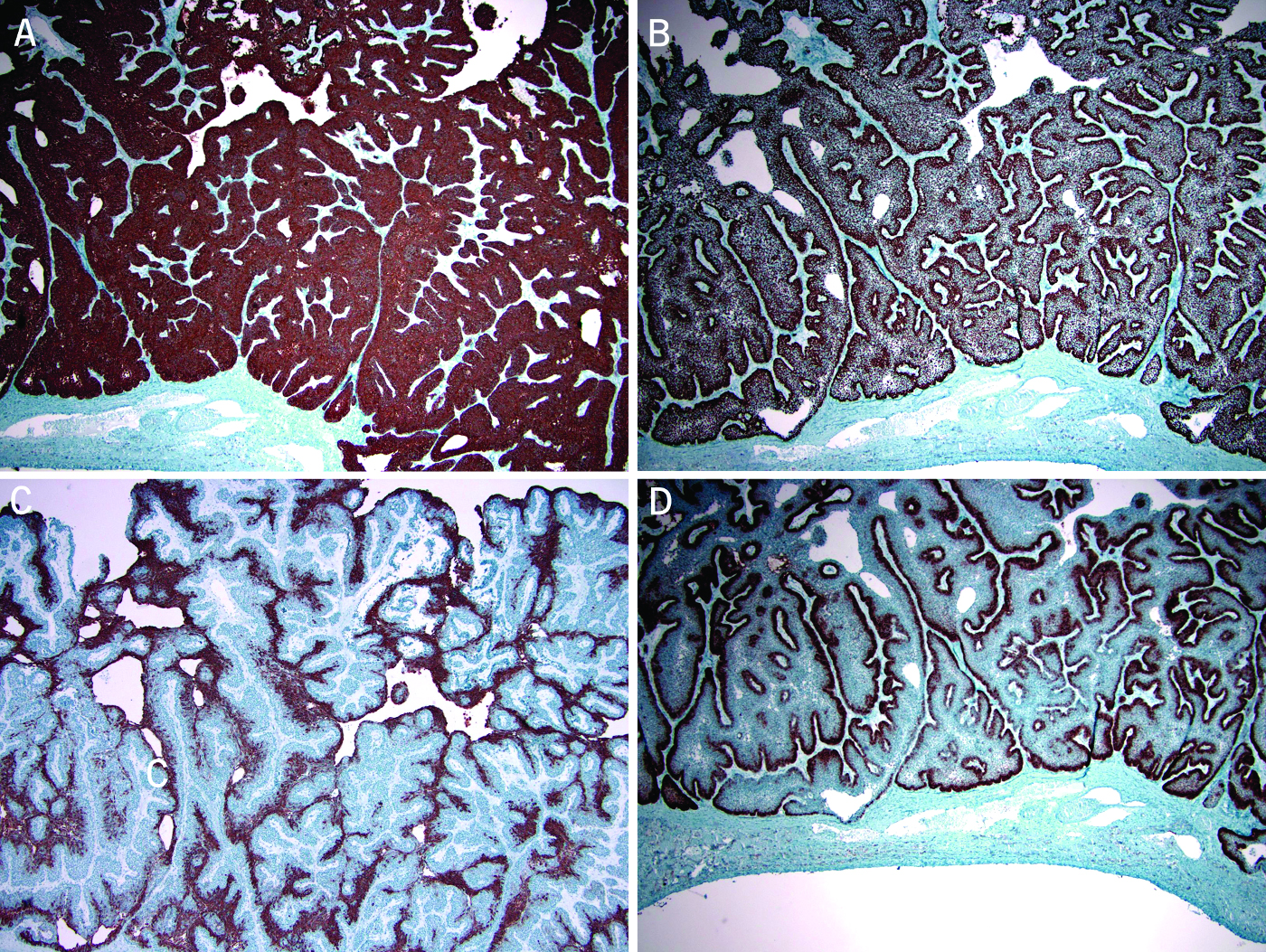
Figure 3. Immunohistochemical stains show the tumor cells were positive for CK5/6 (A, peroxidase stain 40X) and p63 (B, peroxidase stain 40X). The squamoid cells in the central portion of the islands were positive for CK19 (C, peroxidase stain 100X). The peripherally palisading cells were strongly positive for CD10 (D, peroxidase stain 40X).
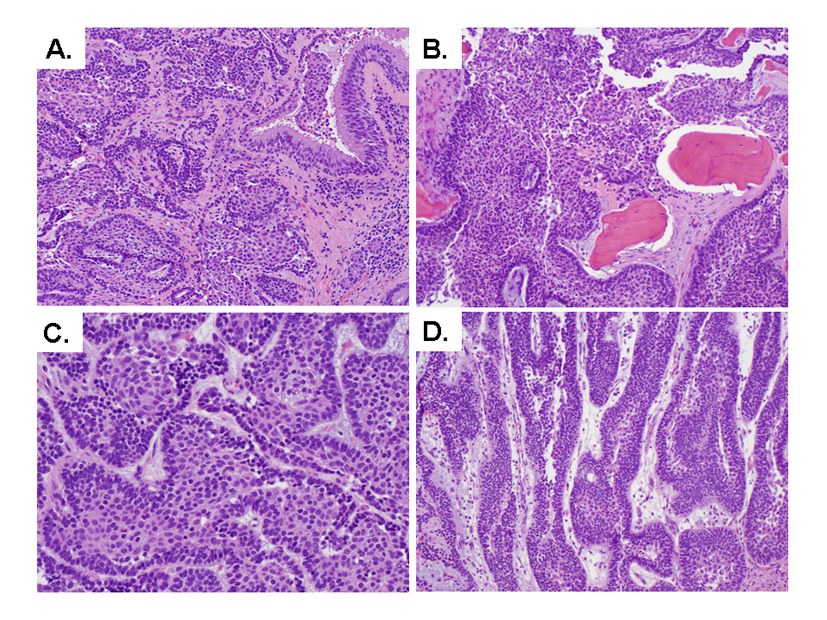
Figure 4. Microscopic features of the resected nasal mass (A-D). (A) Tumor invades nasal mucosa (H&E stain, 100X). (B) Tumor permeates maxillary bone (H&E stain, 100X). (C) Interlocking islands consisted of peripheral palisading of basaloid cells (H&E stain, 400X). (D) Focal plexiform configuration (H&E stain, 200X).