Figures
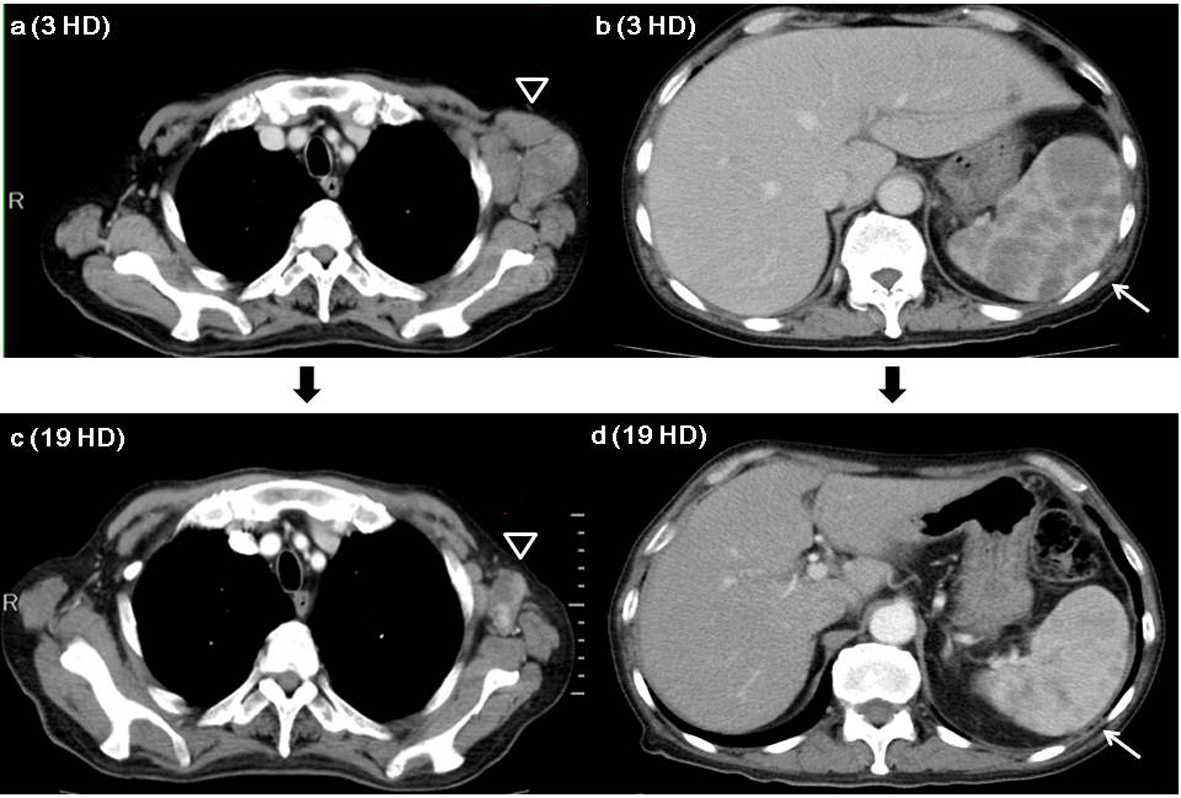
Figure 1. Enhanced chest and abdominal CT series. a). Chest CT on 3 HD showing enlarged left axillary lymph nodes (open triangle). b). Abdominal CT on 3 HD showing multiple low-contrast nodules in the enlarged spleen (arrow). c). Chest CT on 19 HD showing left axillary lymph nodes (open triangle) were smaller compared to the findings of chest CT on 3 HD. d). Abdominal CT on 19 HD showing low-contrast nodules have disappeared from the spleen (arrow). Abbreviations: HD; hospital day.
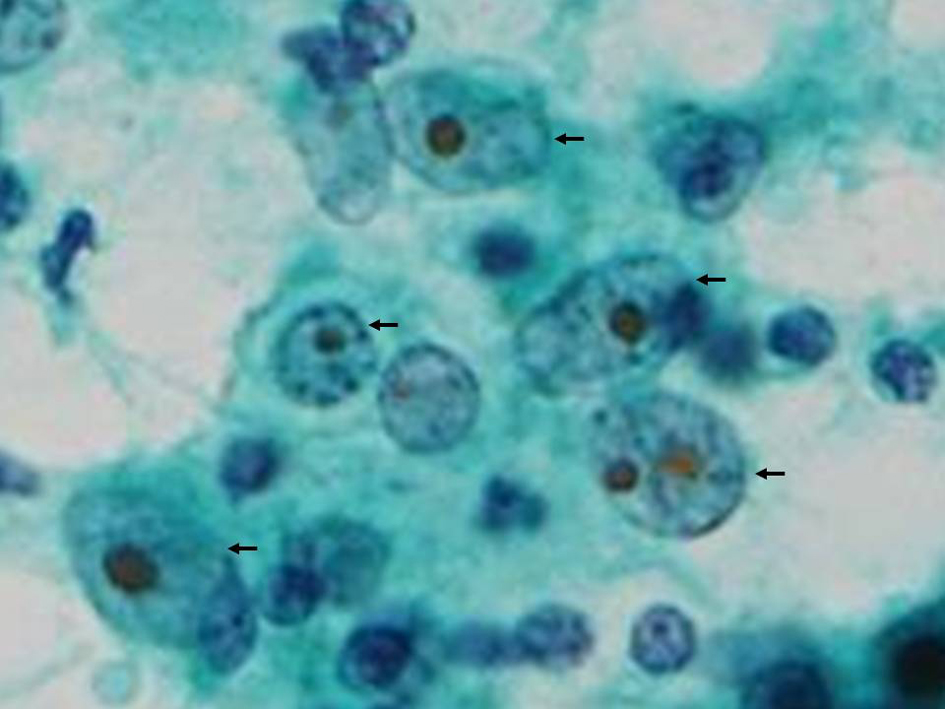
Figure 2. Aspiration cytology of left axillary lymph nodes. Aspiration cytology showing large atypical cells (arrows) with big nuclear body indicative class V. Original magnification, × 400, Papanicolaou stain.
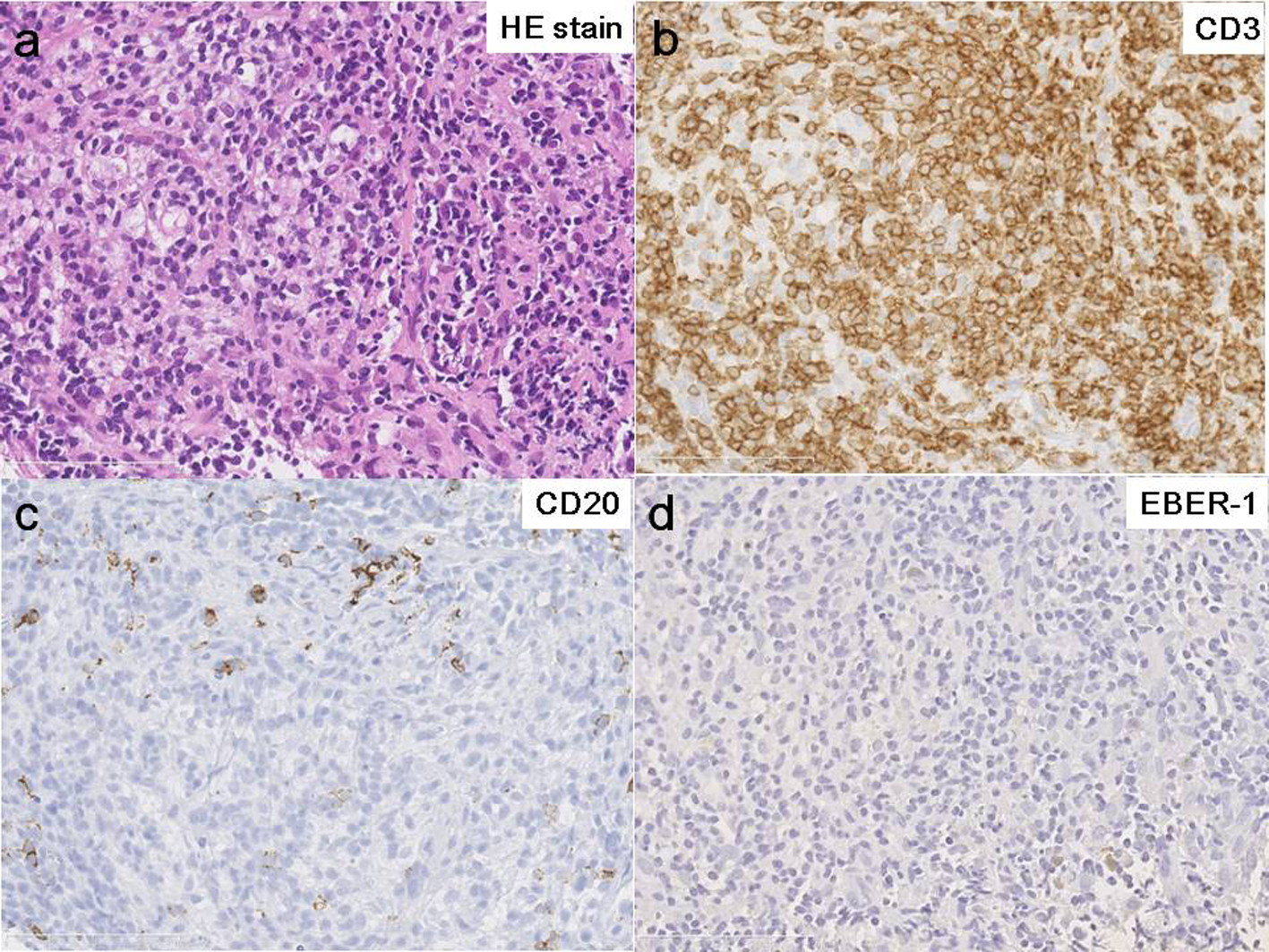
Figure 3. Pathology of axillary lymph nodes. Histology of biopsy specimens (HE staining) showing angioimmunoblastic lymphadenopathy-type lymphoproliferative disorder (a) including cells that were diffusely positive for T-cell marker (CD3) (b), and a few cells that were weakly positive for B-cell marker (CD20) (c) immunohistochemically and negative for EBV-encoded RNA (EBER-1) by in situ hybridization staining (d). These pathological features mimic peripheral T-cell lymphoma. Original magnification, × 400.
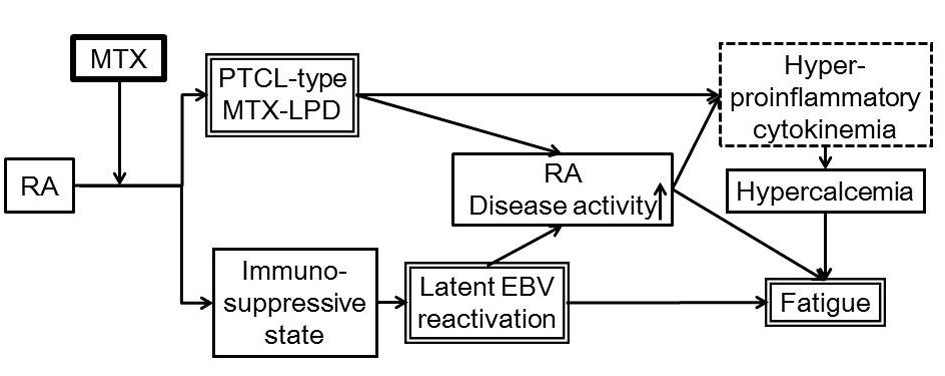
Figure 4. Proposed pathogenic relationship among RA, MTX-LPD, hypercalcemia and general malaise in our patient. We propose that the immuno-suppressive state induced by MTX treatment for RA reactivated latent EBV and possibly coincidentally was associated with PTCL-type MTX-LPD. Hyperproinflammatory cytokinemia resulting from both high disease activity of RA and PTCL-type MTX-LPD caused hypercalcemia and consequent fatigue. Abbreviations: RA: Rheumatoid arthritis; MTX: Methotrexate; EBV: Epstein-Barr virus; PTCL: peripheral T-cell lymphoma; MTX-LPD: Methotrexate - lymphoproliferative disease.
Table
Table 1. Summary of the Investigations Performed, all Positive and Relevant Negative Results are Shown
| Urinalysis on admission: | Biochemistry on admission: | Hormone test on admission: |
|---|
| CBC: complete blood count; ESR: erythrocyte sedimentation rate; EBV: Epstein-Barr virus; EBV-EBNA: anti-EBV associated nuclear antigen; EBV-VCA: anti-EBV capsid antigen; PTHrP: parathyroid hormone-related protein; iPTH: intact parathyroid hormone; HCV: Hepatitis C virus; HTLV-1: Human T-lymphotropic virus Type I. |
| pH | 5.0 | | TP | 5.9 | g/dL | 1, 25-dihydroxy vitamin D3 | 17 | pg/dL |
| Specific Gravity | 1.020 | | Alb | 1.9 | g/dL | PTHrP | 1 | pmol/L |
| Protein | ± | | AST | 54 | U/L | iPTH | < 5 | pg/mL |
| Sugar | - | | ALT | 52 | U/L | |
| Acetone | - | | LDH | 205 | U/L | Viral antibody test on admission: |
| Bilirubin | - | | CK | 13 | U/L | HCV antibody | negative | |
| Urobilinogen | ± | | ALP | 274 | U/L | HTLV-1 antibody | negative | |
| Occult blood | ± | | CRP | 22.8 | mg/dL | | |
| CBC on admission: | Na | 140 | mmol/L | EBV studies on hospital day 22: |
| White Blood Cell | 11,250 | /µL | K | 3.8 | mmol/L | EBV-VCA IgG | 1,280 | times |
| Neutrophil | 93.0 | % | Cl | 101 | mmol/L | EBV-VCA IgM | < 10 | times |
| Lymphocyte | 2.0 | % | Ca | 10.2 | mg/dL | EBV-EBNA IgG | 10 | times |
| Monocyte | 5.0 | % | P | 6.0 | pg/mL | EBV DNA | 1.4 × 103 | copies/106 cells |
| Red Blood Cell | 585 × 104 | /µL | BUN | 42 | mg/dL | |
| Hb | 15.5 | g/dL | Cr | 1.69 | mg/dL | EBV studies on 72 days after discharge: |
| Platelet | 39.6 × 104 | /µL | | | | EBV-EBNA IgG | 40 | times |
| ESR | 135 | mm/hr | | | | EBV DNA | 1.1 × 102 | copies/106 cells |