
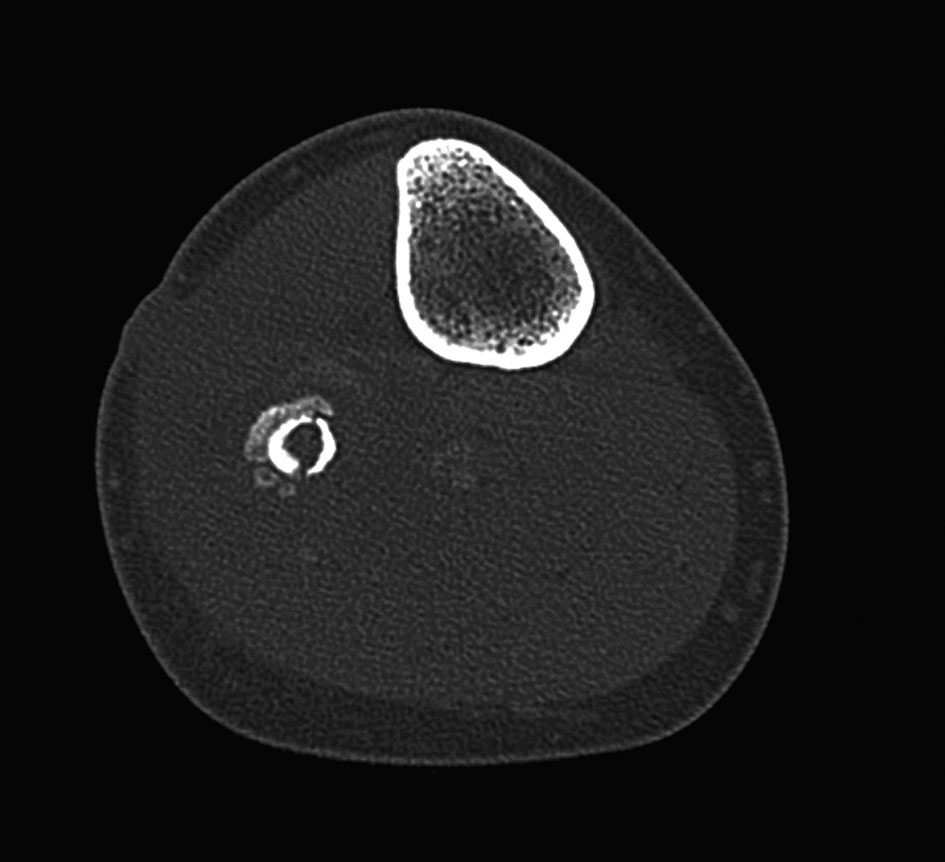
Figure 1. X-ray of the fibula of our patient at initial presentation without signs of osteomyelitis.
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 3, Number 1, February 2012, pages 7-11
A Case of Sequester and Involucrum Formation of the Fibula
Figures

Table
| Anatomic type | Physiologic host |
|---|---|
| 1: Medullary osteomyelitis. Nidus is endosteal. | A: Normal host/immune system/vascularity. |
| 2: Superficial osteomyelitis. Limited to the surface of the bone. | B: Bs systemic compromise. B1 local compromise. Bs1 systemic and local compromise. |
| 3: Localized osteomyelitis. Full thickness of the cortex is involved. | C: Treatment morbidity worse than present condition. |
| 4: Diffuse osteomyelitis. Entire circumference involvement. |