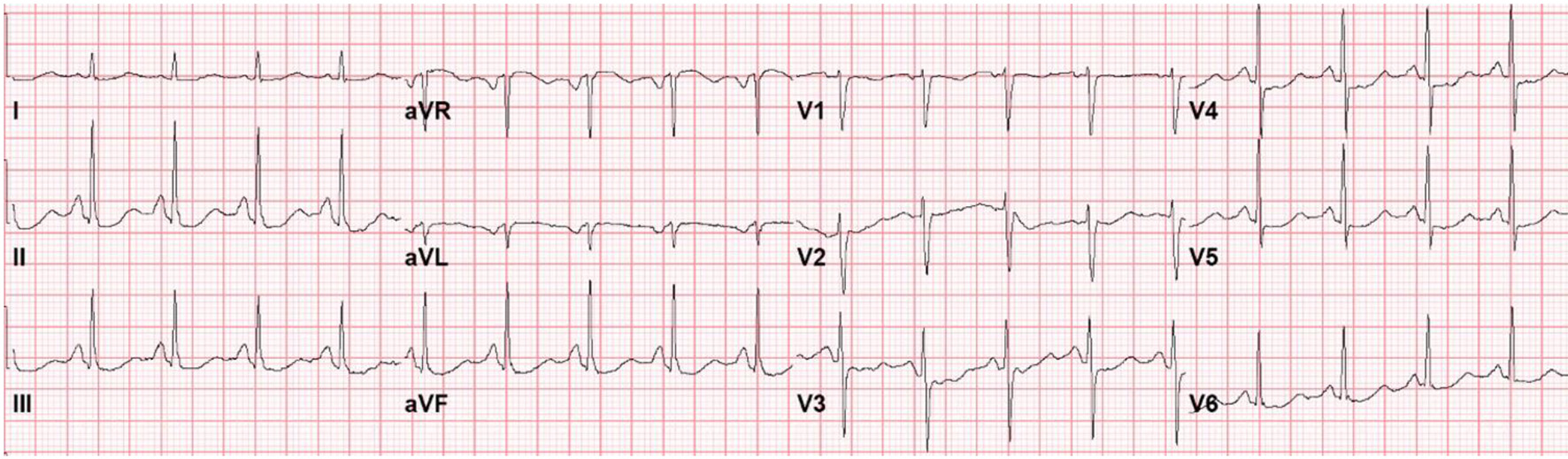
Figure 1. Electrocardiogram on presentation to the emergency department with seizure-like activity, headache, nausea, vomiting, diarrhea, and severe fatigue.
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://www.journalmc.org |
Case Report
Volume 13, Number 6, June 2022, pages 263-268
Takotsubo Cardiomyopathy Secondary to Cryptococcal Meningoencephalitis in a Patient With Multiple Sclerosis
Figures
Table
| Lab | Value | Reference range |
|---|---|---|
| Hemoglobin | 11.4 g/dL | 11.1 - 15.9 |
| Hematocrit | 32.7% | 34 - 46.6 |
| White blood cell | 20.8 × 103/µL | 3.4 - 10.8 |
| Platelets | 141 × 103/µL | 150 - 450 |
| Sodium | 128 mEq/L | 134 - 144 |
| Potassium | 2.5 mEq/L | 3.5 - 5.3 |
| Chloride | 88 mEq/L | 98 - 109 |
| Creatinine | 0.64 mg/dL | 0.57 - 1.00 |
| Blood urea nitrogen | 12 mg/dL | 7 - 25 |
| Calcium | 8.9 mg/dL | 8.7 - 10.3 |
| Glucose | 200 mg/dL | 70 - 99 |
| Lactic acid | 2.2 mmol/L | 0.5 - 2.2 |