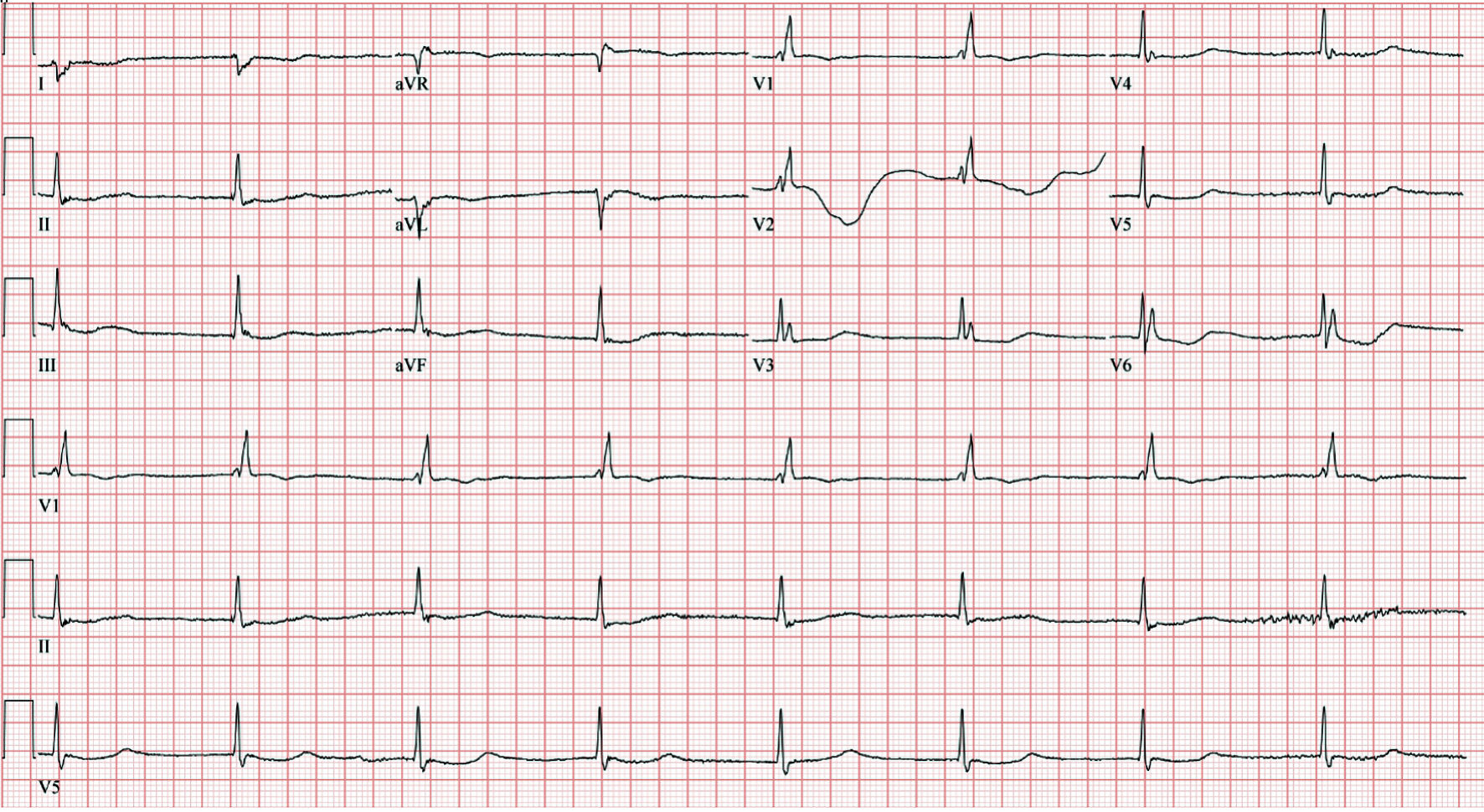
Figure 1. ECG on admission demonstrated a junctional escape rhythm with right bundle branch block, 47 beats/min ventricular rate, and QTc of 509 ms. ECG: electrocardiogram.
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://www.journalmc.org |
Case Report
Volume 13, Number 7, July 2022, pages 341-348
The Ominous Triad of Severe Takotsubo Cardiomyopathy
Figures
Tables
| Laboratory test | Patient’s result | Reference range |
|---|---|---|
| White cells count (WCC) | 10 × 103/µL | 3.3 - 10.7 × 103/µL |
| Hemoglobin | 12.2 g/dL | 12.1 - 15.0 g/dL |
| Mean corpuscular volume (MCV) | 95 fL | 80 - 100 fL |
| Platelets | 286 × 103/µL | 150 - 400 × 103/µL |
| Serum sodium | 138 mmol/L | 133 - 144 mmol/L |
| Serum chloride | 99 mmol/L | 98 - 107 mmol/L |
| Serum potassium | 3.9 mmol/L | 3.5 - 5.2 mmol/L |
| Serum bicarbonate | 20 mmol/L | 21.0 - 28.0 mmol/L |
| Anion gap | 13 mEq/L | 3 - 11 mEq/L |
| Serum calcium | 8.9 mg/dL | 8.6 - 10.8 mg/dL |
| Serum magnesium | 1.3 mg/dL | 1.6 - 3.0 mg/dL |
| Blood urea nitrogen (BUN) | 31 mg/dL | 9.0 - 25.0 mg/dL |
| Serum creatinine | 1.34 mmol/L | 0.5 - 1.2 mmol/L |
| Serum glucose | 158 g/dL | 70 - 140 g/dL |
| Aspartate aminotransferase (AST) | 87 U/L | 7 - 52 U/L |
| Alanine aminotransferase (ALT) | 51 U/L | 13 - 39 U/L |
| International normalized ratio (INR) | 1.07 | < 1.1 |
| Lactic acid | 3.7 mmol/L | 0.5 - 2.2 mmol/L |
| High-sensitivity troponin I | 17 ng/mL | 0 - 0.4 ng/L |
| Brain natriuretic peptide (BNP) | 249 pg/mL | < 450 pg/mL |
| Thyroid-stimulating hormone (TSH) | 3.95 µIU/mL | 0.5 - 5 µIU/mL |
| Hospital staya | Time | HR (beats/min) | QTc (ms) |
|---|---|---|---|
| aPatient was admitted at 16:25. Notice the resolution of QTc interval prolongation following temporary venous pacing (TVP) with a programed lower rate limit (LRL) of 70 beats/min. QTC: corrected QT interval. | |||
| Day 1 | 16:28 | 47 | 509 |
| 16:31 | 46 | 519 | |
| 17:00 | 41 | 537 | |
| 17:49 | 41 | 545 | |
| 17:50 | 41 | 536 | |
| 18:05 | 67 | 407 | |
| Day 2 | 16:20 | 85 | 466 |
| 16:21 | 67 | 405 | |
| 22:00 | |||
| Article | Age/sex | Past medical history | ECG rhythm on admission | Duration of QT interval on admission ECG | TTE findings | Timing of NA or CA | Rhythm causing NA or CA | Temporality of TTE findings with TdP and/or CA | Timing of PPP |
|---|---|---|---|---|---|---|---|---|---|
| ECG: electrocardiogram; VF: ventricular fibrillation; CV: cardioversion; EJR: escape junctional rhythm; HB: heart block; RBBB: right bundle branch block; AVB: atrioventricular block; TWI: T wave inversion; VR: ventricular rate; PVC: premature ventricular contractions; TdP: torsade de pointes; TTE: transthoracic echocardiogram; b/min: beats/min; HTN: hypertension; TVP: temporary venous pacing; PPP: permeant pacemaker placement; LAFB: left anterior fascicular block; LVEF: left ventricular ejection fraction. | |||||||||
| Ahn et al, 2011 [27] | 78/F | HTN | Third-degree HB with EJR of 35 b/min, combined with TWI precordial leads | 580 ms | Akinesia of mid and apical LV walls with the systolic ballooning of the ventricular apex; LVEF: 35% | 24 - 48 h | Third-degree HB with EJR of 20 b/min QTc 720 ms followed by TdP (treated by CV and TVP) | Before | Day 21 |
| de Santana et al, 2021 [24] | 56/F | HTN, grade 2 obesity | Second degree AVB 2:1 with EJR of 50 b/min, RBBB, LAFB, biphasic and inverted T waves in precordial and limb leads | 689 ms | Basal hypercontractility and midventricular and apical ballooning. LVEF: 40% | 24 h | VF (treated by CV and TVP) | Before | Day 14 |
| Inayat et al, 2017 [8] | 59/F | None | Third-degree AVB with EJ VR 48 b/min, multiple PVCs, prolonged, and deep TWI in limb leads | 643 ms | Basal hyperkinesia and apical hypokinesis with LVEF of 35-40% | 24 - 48 h | TdP (treated medically and TVP) | Before | Day 6 |
| Kurisu et al, 2008 [26] | 87/F | Syncope | RBBB during 2:1 AVB with a VR of 42 b/min, TWI in leads I, II, aVL, aVF and V1 to V6 | 880 ms | Akinesia of the distal portion of the LV chamber, LVEF 62% | Immediately | TdP (treated medically and TVP) | After | Day 10 |
| Kurisu et al, 2008 [26] | 78/F | Not reported | RBBB during complete AVB with a VR of 40 b/min, ST segment elevation in leads V2 to V6, T wave inversion in leads I, II, III, aVF and V1 to V6 | 920 ms | Akinesia of the mid to distal portion of the LV chamber, LVEF 38% | Immediately | TdP (treated medically and TVP) | After | Day 7 |