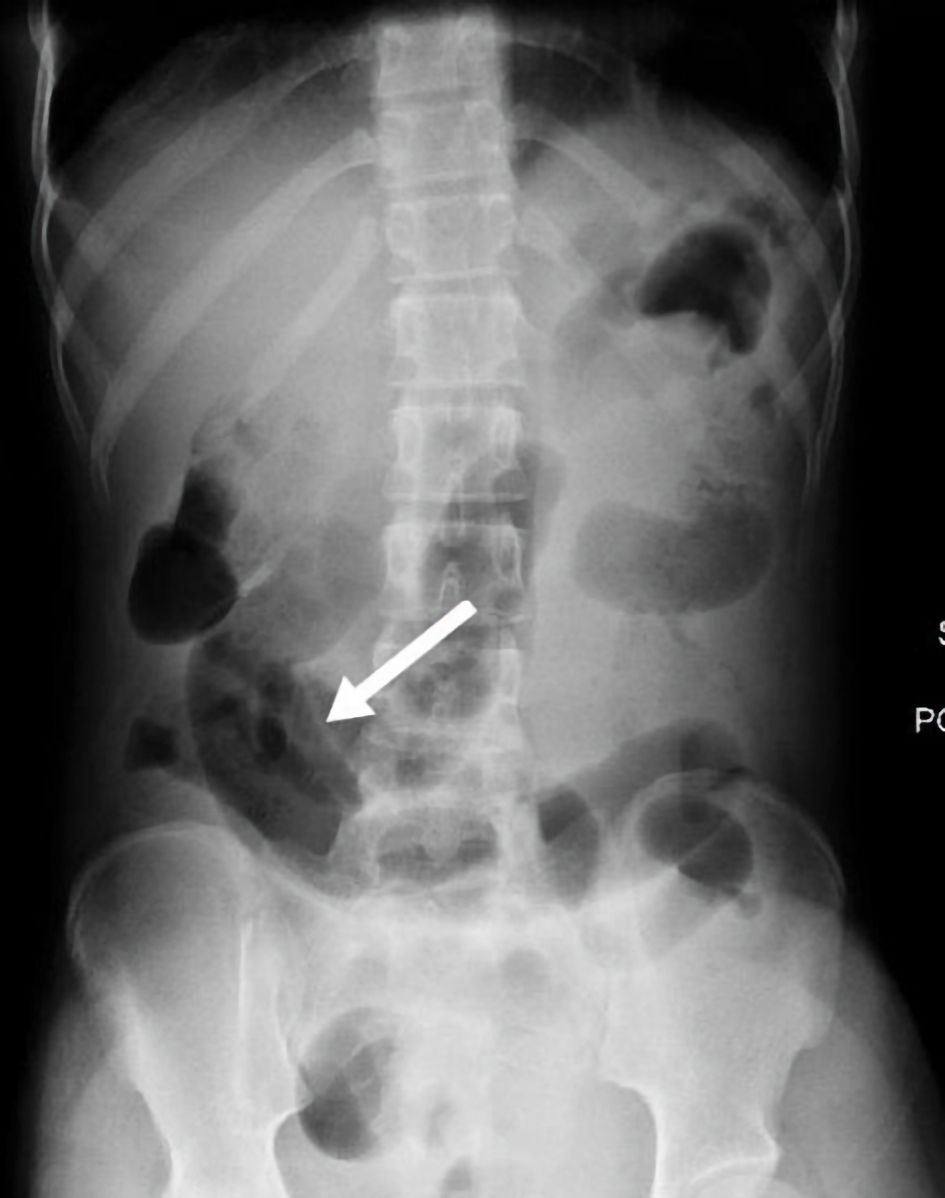
Figure 1. Abdominal X-ray showed moderately distended gas filled loops (white arrow).
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://www.journalmc.org |
Case Report
Volume 13, Number 7, July 2022, pages 335-340
Small Bowel Obstruction and Appendicitis in Patient With Fitz-Hughes-Curtis Syndrome
Figures

Table
| Current case | Khine et al, 2019 [10] (case 1) | Kazama et al, 2013 [11] | Ishimaru et al, 2021 [12] | |
|---|---|---|---|---|
| aPatient was diagnosed with Fitz-Hughs-Curtis syndrome during a laparoscopic examination. bPatient was treated empirically for C. trachomatis with azithromycin and levofloxacin based on CT imaging findings prior to specimen collection. SBO: small bowel obstruction; CT: computed tomography; WBC: white blood cell; N. gonorrhoeae: Neisseria gonorrhoeae; C. trachomatis: Chlamydia trachomatis; PID: pelvic inflammatory disease. | ||||
| Age (years) | 15 | 16 | 27 | 22 |
| Symptoms | Nausea and vomiting | Abdominal pain | Abdominal pain | Vomiting and abdominal pain |
| Fever | Afebrile | Afebrile | Low-grade fever | Febrile |
| Location of abdominal pain | Diffuse | Left lower quadrant | Right upper quadrant | Lower abdomen/right flank |
| Vaginal discharge | None | None | Increased | Vaginal discharge 3 months prior |
| CT imaging | No peritoneal or capsular enhancement | Not reporteda | Hepatomegaly, capsular enhancement, enlarged appendix with wall thickening | Enlarged appendix with surrounding fat stranding |
| Pelvic ultrasound | Complex bilateral ovarian cysts and normal reproductive anatomy | Left ovarian mass | Unremarkable | Not reported |
| Laboratory results | Leukocytosis, elevated platelets, neutrophilia (80%), and hyponatremia | Not reported | Elevated C-reactive protein, elevated WBC | Elevated C-reactive protein, elevated WBC, neutrophilia |
| Liver enzymes | Not elevated | Not reported | Slightly elevated | Not elevated |
| Pathogen: N. gonorrhoeae or C. trachomatis | C. trachomatis | C. trachomatis | Negativeb | C. trachomatis |
| Laparoscopic findings | Chronic thickening of the appendix, adhesions on left and right liver lobesa | PID with extensive adhesions, bilateral pyosalpinxes, left ovarian abscess, and perihepatic inflammation with classic violin string signs | No surgical intervention | Inflammation of appendix, bloody ascites, adhesionsa |
| Complications SBO and/or appendicitis | SBO and appendicitis | Not reported | Appendicitis | Appendicitis |