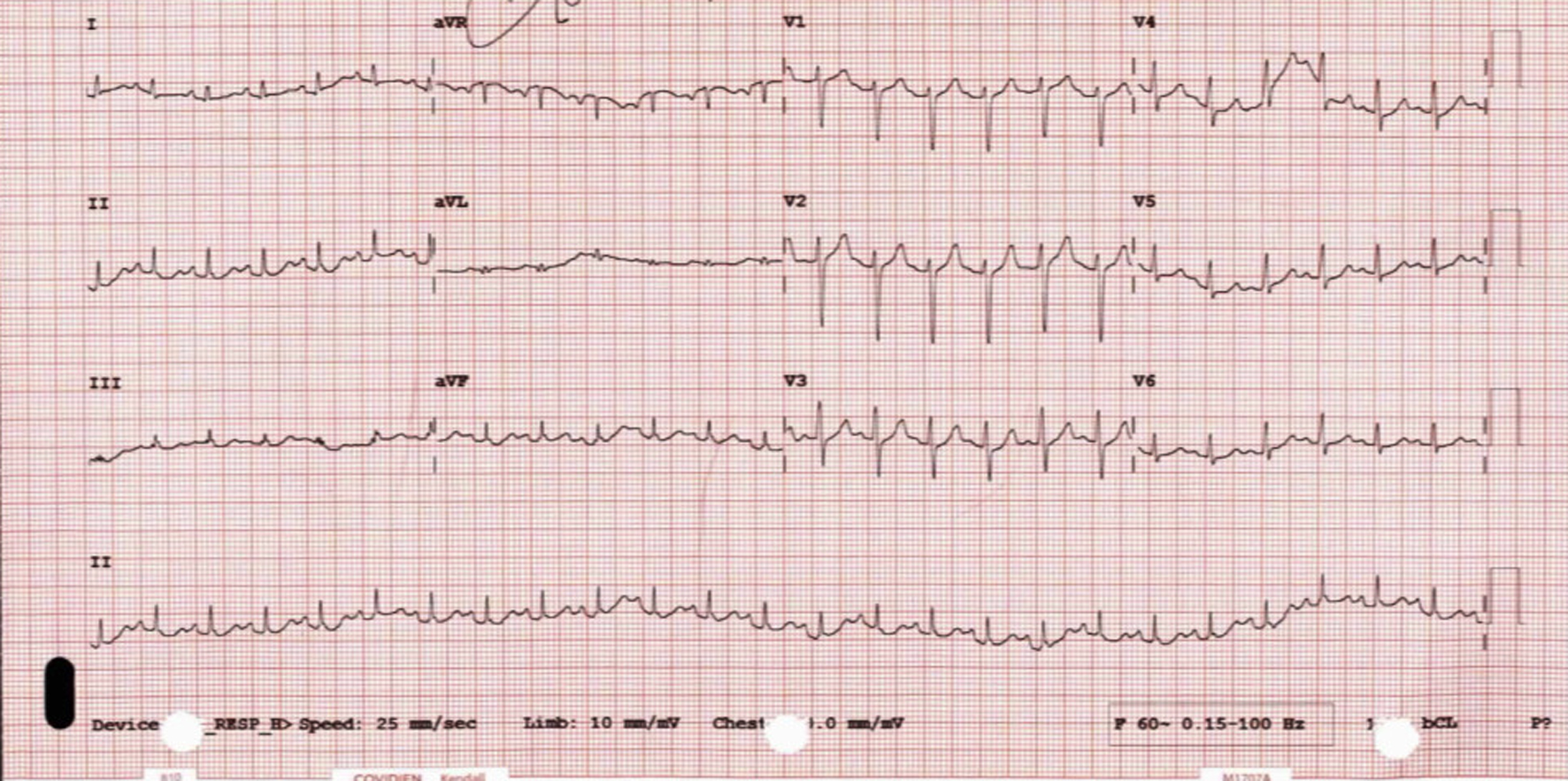
Figure 1. ECG: sinus tachycardia, no significant ST-segment changes. ECG: electrocardiogram.
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://www.journalmc.org |
Case Report
Volume 13, Number 8, August 2022, pages 414-420
Reverse Takotsubo Cardiomyopathy in a Patient With Commotio Cordis
Figures
Table
| Variants | Prevalence |
|---|---|
| MLV: mid-left ventricular; CMR: cardiac magnetic resonance. | |
| Apical with or without MLV variant (typical) | 75-80% |
| MLV | About 10-15% |
| Inverted or basal | About 5% |
| Biventricular | Clinical < 0.5%; CMR 33% |
| Right ventricular | Unknown |
| Apical tip sparing | Unknown |
| Possible atypical variants | |
| Global | Unknown |
| Focal | Unknown |