
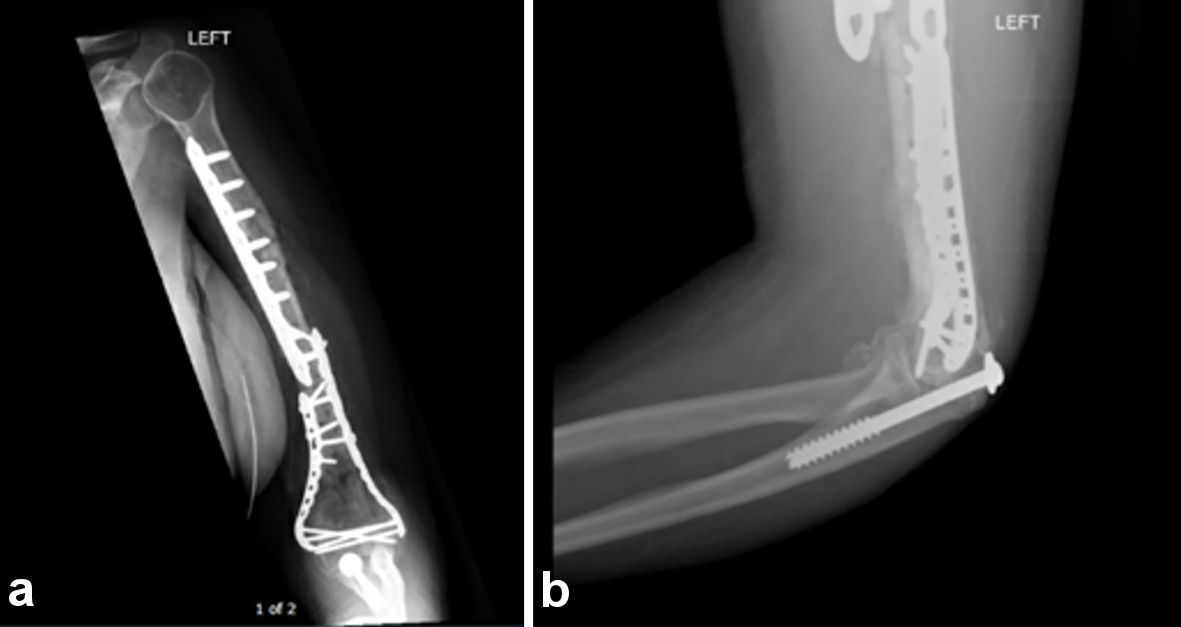
Figure 1. (a) The initial radiograph diagnosing the absence of a 6-inch humeral diaphysis. (b) Extruded fragment of bone present in the hands of emergency department personnel immediately following the MVC.
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://www.journalmc.org |
Case Report
Volume 13, Number 8, August 2022, pages 408-413
Traumatic Humeral Diaphysis Extrusion and Replantation With Periosteal Involvement
Figures

Table
| Name of study | Involved bone | Preparation techniques | Results of implantation | Other notes |
|---|---|---|---|---|
| Traumatic femoral bone loss [1] | Large femur fragment (10 inches) | Cultured, autoclaved, and treated with betadine | No infection, 2 years later patient walked with a barely noticeable limp | Negative for neurovascular injury, intact periosteal sheath and vasculature |
| Traumatic femoral bone defect reconstruction [6] | Large femur fragment (11 cm) | Autoclave at 121 °C, for 20 min at 1.3 bars | Complete healing of both fracture lines at 2 years follow-up | Intact periosteal sheath and vasculature |
| Head-on allograft transplantation [4] | Multiple small femur fragments | Discarded fragments, due to the high risk of nonunion | Allograft utilized | Far too much fragmentation |