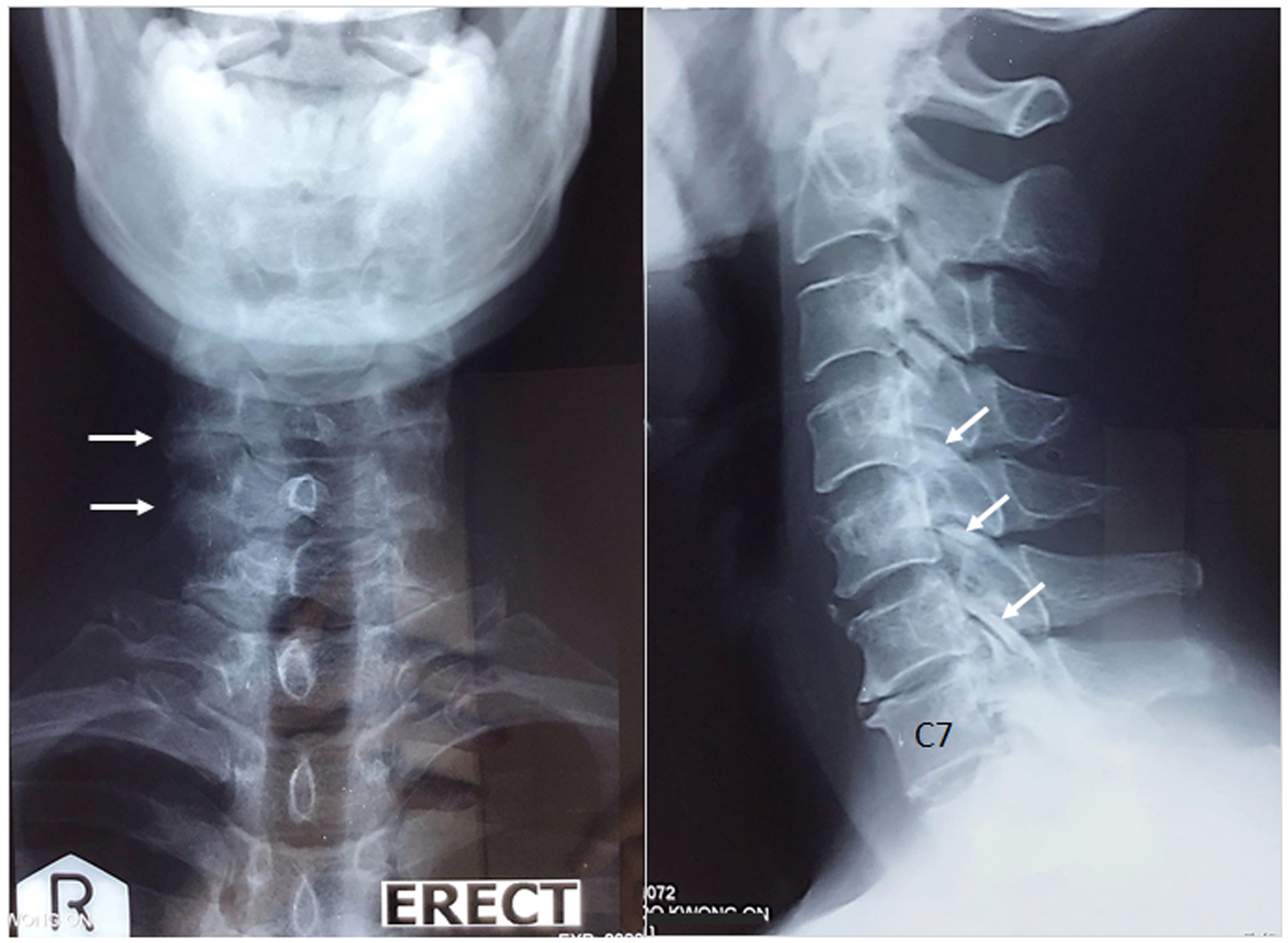
Figure 1. Anterior and lateral views of the cervical spine. Cervical radiographs show narrowed interspaces from C4/C5 to C7/T1 levels, anterior osteophytic lipping of the cervical vertebrae, degenerative hypertrophy of the facet joints (white arrows), and calcified discs of the C2/C3 and C4/C5 spaces. The radiographic findings are consistent with degenerative spondylosis.
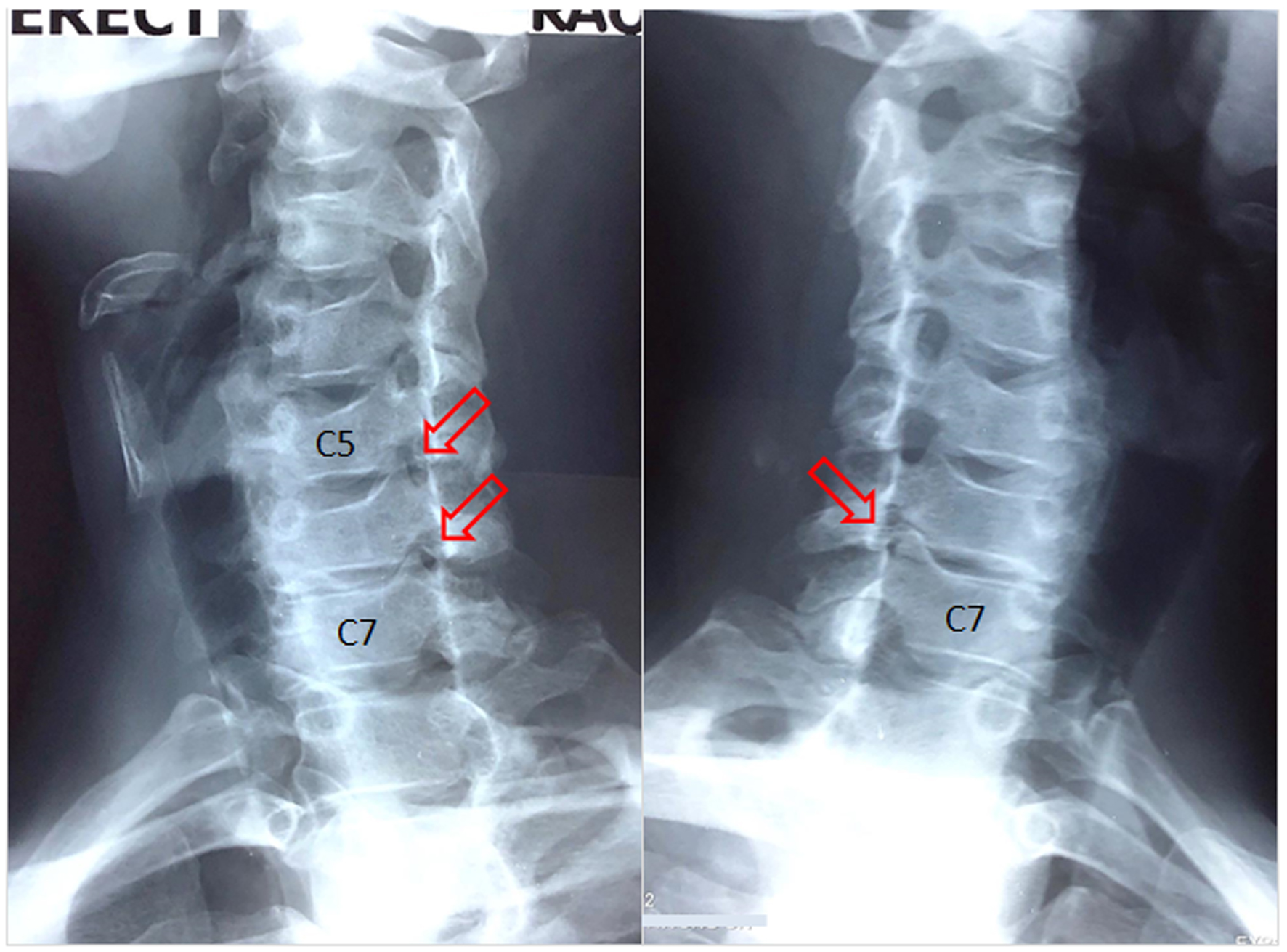
Figure 2. Oblique radiographs of the cervical spine demonstrate neuroforaminal stenosis with posterior osteophyte encroachment at the right C5/C6 and bilateral C6/C7 levels (red arrows), consistent with the impression of cervical radiculopathy.
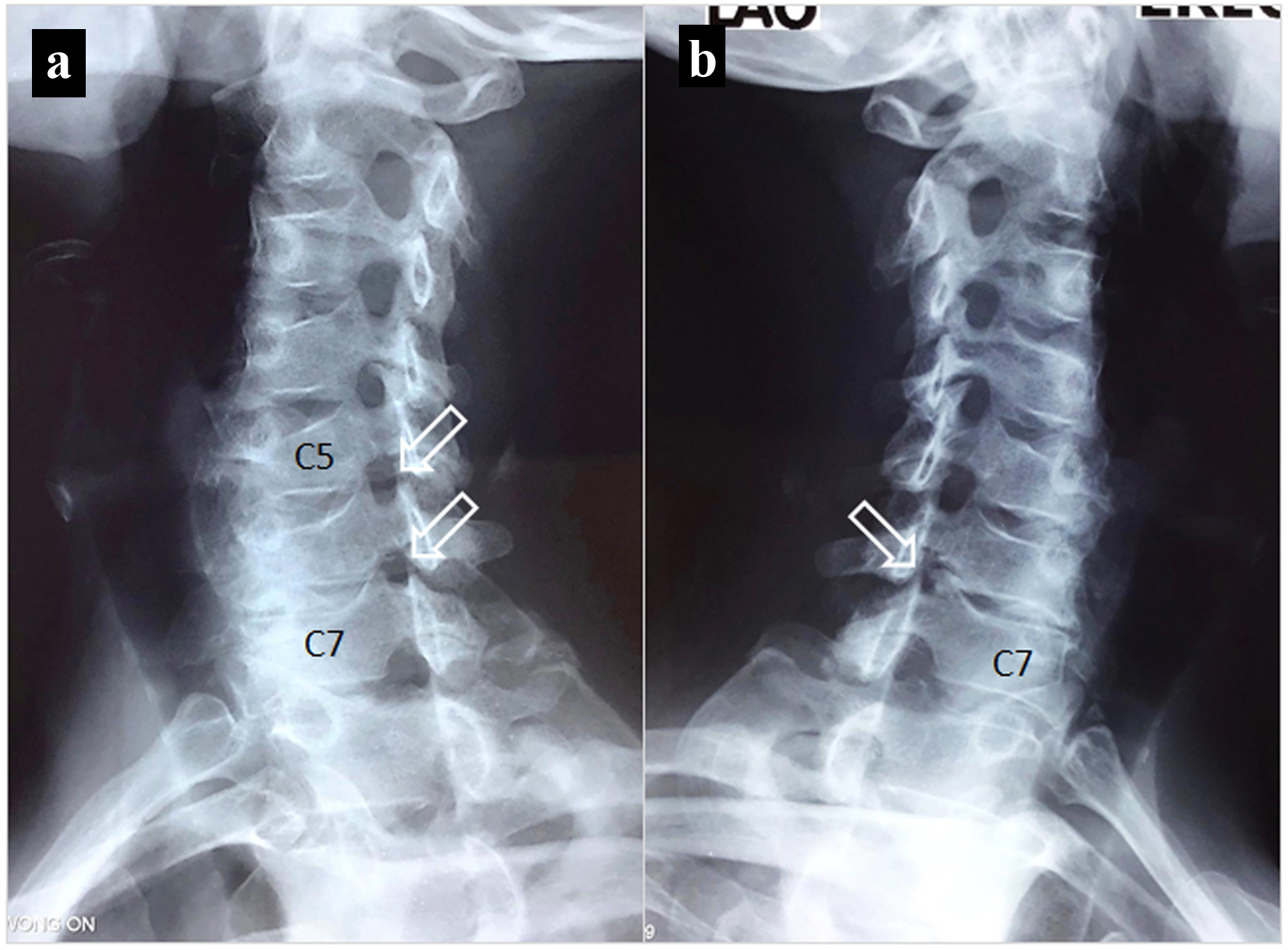
Figure 3. Images obtained 11 months following treatment. (a) The neuroforamina of the right C5/C6 and C6/C7 levels are opened (white arrows). (b) The restricted left C6/C7 opening has greater space than the original finding in Figure 2 on visual assessment. An increase in the spacing of the previously restricted neuroforamina could signify a beneficial alteration related to cervical function improvement.