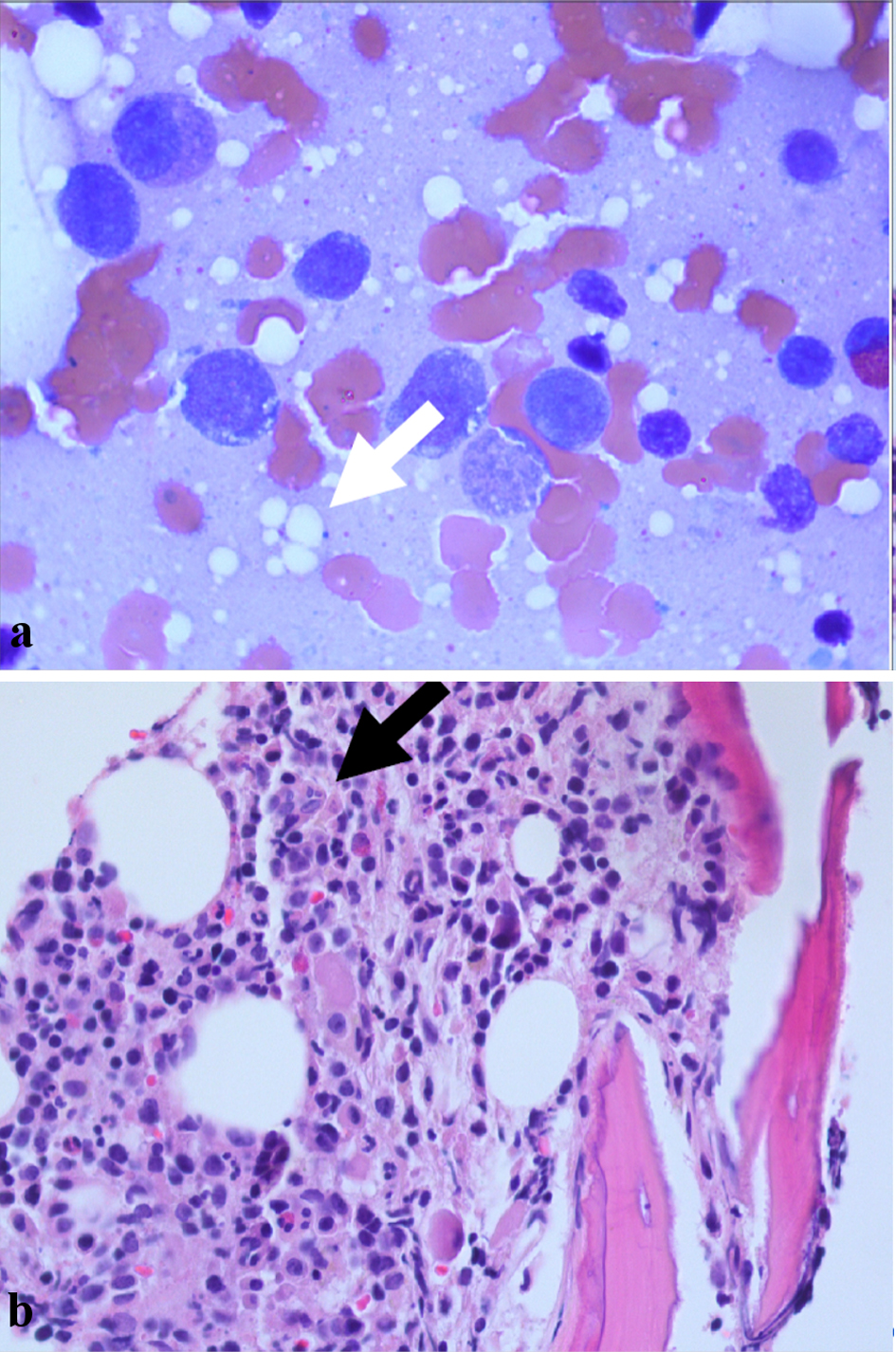
Figure 1. (a) Bone marrow biopsy showing numerous precursor cells including metamyelocytes and promyelocytes with intracellular vacuoles (white arrow). (b) Bone marrow biopsy showing hypercellular bone marrow (black arrow).
| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://www.journalmc.org |
Case Report
Volume 14, Number 9-10, October 2023, pages 327-331
A Double Hit to Ubiquitination Leading to a New Diagnosis of VEXAS Syndrome
Figure
Tables
| Lab | Value | Reference range |
|---|---|---|
| WBC: white blood cell; Hb: hemoglobin; MCV: mean corpuscular volume; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein. | ||
| WBC | 14.3 g/dL | 4.5 - 11 × 103 g/dL |
| Hb | 10.1 g/dL | 12 - 17.5 g/dL |
| MCV | 100.8 fL | 80.0 - 100.0 fL |
| Platelet | 232 × 103/µL | 140 - 450 × 103/µL |
| Lymphocytes | 12.2% lymphocytes | 25.0-43.0% |
| Metamyelocytes | 3.5% | 0% |
| Myelocytes | 3.5% | 0% |
| Promyelocytes | 0.9% | 0% |
| Iron | 40 | 45 - 180 µg/dL |
| Ferritin | 1,042.9 | 22 - 335 ng/mL |
| Transferrin | < 70 | 215 - 365 mg/dL |
| ESR | 90 | 0 - 20 mm/h |
| CRP | 49 | 0 - 10 mg/L |
| Lab | Value | Reference range |
|---|---|---|
| TPO: thyroperoxidase; RNP: ribonucleoprotein; Hb: hemoglobin; G6PD: glucose-6-phosphate dehydrogenase; PNH: paroxysmal nocturnal hemoglobinuria. | ||
| TPO | 114 | < 9 IU/mL |
| RNP | 3 | 0.0 - 0.9 AI |
| G6PD | 23.8 | 7.0 - 20.5 U/g Hb |
| PNH assay | No flow cytometric evidence | Negative |