

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 7, Number 12, December 2016, pages 522-523
Hydatid Disease in the Gallbladder: A Rare Location
Mustafa Yener Uzunoglua, Fatih Altintoprakb, c, Enis Dikiciera, Ismail Zengina, Ahmet Celika
aDepartment of General Surgery, Sakarya University Research and Educational Hospital, Adapazari, Turkey
bDepartment of General Surgery, Sakarya University Faculty of Medicine, Adapazari, Turkey
cCorresponding Author: Fatih Altintoprak, Department of General Surgery, Sakarya University Faculty of Medicine, Adapazari, Turkey
Manuscript accepted for publication May 11, 2016
Short title: Hydatid Disease
doi: https://doi.org/10.14740/jmc2501w
| Abstract | ▴Top |
Hydatid cysts, a zoonosis, are endemic to certain geographical regions. These cysts occur most frequently in the liver and lungs. While a hydatid cyst can occur almost anywhere, a primary hydatid cyst of the gallbladder is very rare. A 68-year-old male was admitted to the emergency service with a 2-day history of increasing abdominal pain. The physical examination showed widespread tenderness and guarding, and Murphy’s sign was positive. Following ultrasound examination, the patient underwent surgery with a preliminary diagnosis of acute cholecystitis. A primary hydatid cyst of the gallbladder was detected, and the patient underwent a cholecystectomy. A primary hydatid cyst of the gallbladder has not been diagnosed previously with gallbladder disease; in such a case, there are no cysts at any location other than the gallbladder. This paper presents a rare case to emphasize the difficulty of diagnosing a primary hydatid cyst of the gallbladder preoperatively.
Keywords: Acute cholecystitis; Hydatid cyst; Cholecystectomy
| Introduction | ▴Top |
Hydatid cysts are a major cause of morbidity and mortality in many parts of the world. The major cause of this disease is the flatworm Echinococcus granulosus [1]. While more frequent in regions where sheep are raised, E. granulosus has a broad geographical distribution. Pathologies of the gallbladder, on the other hand, are frequent in all societies, and pathologies originating from the gallbladder, particularly acute cholecystitis, are major causes of admission to emergency services.
A primary hydatid cyst of the gallbladder has not been diagnosed previously with gallbladder disease; in such a case, there are no cysts at any location other than the gallbladder [2]. It is a rare condition, limited to a few case reports. Here, we present a patient who was admitted with abdominal pain and underwent surgery with a preliminary diagnosis of acute cholecystitis. He was diagnosed with a hydatid cyst of the gallbladder intraoperatively. The literature on hydatid cysts of the gallbladder is reviewed.
| Case Report | ▴Top |
A 68-year-old male was admitted to the emergency service with a 2-day history of increasing abdominal pain. The patient had type II diabetes mellitus, and had intermittent, colic-type pain in the right upper quadrant for the past 2 months. On admission, the patient’s blood pressure was 120/80 mm Hg and pulse was 84 beats/min; he was afebrile. The physical examination showed widespread abdominal tenderness, which was more prominent in the right upper quadrant, and guarding. The gallbladder was palpable in the right upper quadrant, and he had a positive Murphy’s sign. Laboratory tests were normal, except leukocytosis (18,000/mm3) and a high γ-glutamyl transferase (GGT, 269 IU/L). The patient’s abdominal radiographs were normal. Abdominal ultrasonography (USG) showed hydrops of the gallbladder (transverse diameter 54 mm), thickening of the gallbladder wall (4 mm), and dense internal echoes in the gallbladder lumen and pericholecystic fluid. Given the clinical and radiological findings, a preliminary diagnosis of acute cholecystitis was considered and the patient was scheduled for medical treatment. He was started on ampicillin/sulbactam 1 g qid and paracetamol 1 tid, intravenously. When the clinical findings did not improve and the leukocytosis increased to 21,000/mm3, surgery was performed. Laparoscopic exploration showed advanced adhesions of the gallbladder and open surgery was chosen. After separating the adhesions, exploration showed marked hydrops of the gallbladder, which was embedded in the hepatic bed. Following the decision to perform an anterograde cholecystectomy, the gallbladder was cut open from the fundus to reduce the gallbladder hydrops and daughter vesicles were seen within the gallbladder (Fig. 1). The patient did not have any other abdominal pathology and underwent a cholecystectomy. The patient did not have any postoperative problems, and was discharged with anti-helminth drug (albendazole) on day 4. After a histopathological examination, the patient was determined as having a hydatid cyst with intraluminal localization in the gallbladder and has now been followed for 6 months without any problems.
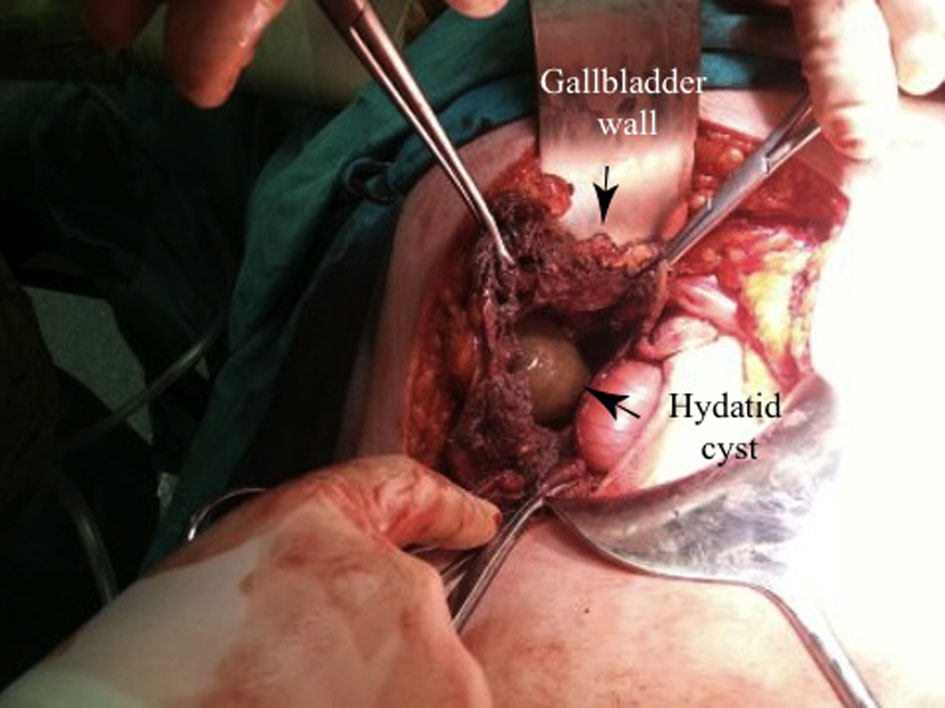 Click for large image | Figure 1. Cyst hydatid vesicle within the gallbladder. |
| Discussion | ▴Top |
Echinococcosis (hydatid disease or hydatidosis) is a parasitic disease, which is seen more frequently in societies in which agriculture and livestock are common practices. A majority of the patients live in rural areas and are involved in raising livestock [3]. Every year, 2 - 3 million new hydatid cyst cases are reported worldwide [2]. It is especially prevalent in South America, Russia, Australia, New Zealand, and Mediterranean countries, where sheep and cattle breeding are common [3]. Hydatid disease is also common in Turkey, with a prevalence of 5.7/100,000 or 2,000 cases/year [4].
While the liver (70-80%) and lungs (15-25%) are the most frequent sites of hydatid cysts, the involvement of other organs is also possible. The exact incidence of extrahepatic cysts is not known, and rare sites include the thyroid, cerebellum, and bone [5]. The gallbladder is an unusual location for primary hydatid disease, with a few reported cases [2, 5, 6]. The unusual sites of hydatid cysts support the hypothesis that parasite embryos, in addition to the portal circulation, can spread via the lymphatic system and bile tract or via daughter vesicles openings into the peritoneal or other spaces [2].
There are several hypotheses regarding the pathogenesis of disease primarily localized in the gallbladder. Spread via the biliary tract is hypothesized for intraluminal cysts, whereas spread via the lymphatic system is considered for extraluminal cysts. Our patient had an intraluminal hydatid cyst.
Hydatid cysts of the liver can remain asymptomatic for long periods due to the slow growth of the cyst, while this period might be shorter for hydatid cysts of the gallbladder, especially for intraluminal cysts. The volume of the gallbladder is much smaller than that of the liver, so clinical symptoms are more likely after a short latency period. While the period between the infestation and clinical symptoms is not known, when the few case reports are examined, the major complaint appears to be abdominal pain. Generally, abdominal pain has a mid-abdominal localization, is described as a “feeling of discomfort”, and is often confused with dyspeptic complaints. While hydatid cysts of the gallbladder presenting with gallbladder perforation have been reported, jaundice and anaphylactic reactions have not been reported in any of these cases [2, 6]. Similarly, in our case, widespread abdominal pain, which was more prominent in the right upper quadrant, was the major complaint.
Due to its rare nature, clinicians and radiologists rarely consider a primary hydatid cyst of the gallbladder as the initial diagnosis. USG, computed tomography (CT), and magnetic resonance imaging (MRI) can be used for the radiological diagnosis of a hydatid cyst. USG is an affordable imaging method with high diagnostic sensitivity in areas where hydatid cysts are endemic, as well as in patients with a family history. The diagnosis can be supported by methods such as a specific enzyme-linked immunosorbent assay (ELISA) and Western blot serology [7]. The exact diagnosis is made after a histopathological examination.
Our patient was evaluated preoperatively using USG, but the possibility of a hydatid cyst was not considered. This diagnosis was considered intraoperatively and was confirmed with the histopathological examination.
In conclusion, a primary hydatid cyst of the gallbladder is a rare condition, and its preoperative diagnosis requires considerable experience.
Conflicts of Interest
The authors declare no conflicts of interest.
| References | ▴Top |
- Craig PS, McManus DP, Lightowlers MW, Chabalgoity JA, Garcia HH, Gavidia CM, Gilman RH, et al. Prevention and control of cystic echinococcosis. Lancet Infect Dis. 2007;7(6):385-394.
doi - Krasniqi A, Limani D, Gashi-Luci L, Spahija G, Dreshaj IA. Primary hydatid cyst of the gallbladder: a case report. J Med Case Rep. 2010;4:29.
doi pubmed - Hakverdi S, Sayar H, Yaldiz M, Erdogan S, Akansu B, Canda MS. [Unusual localization of echinococcosis in Cukurova (134 cases)]. Turkiye Parazitol Derg. 2009;33(1):77-81.
pubmed - Yazar S. [Cystic echinococcosis in Kayseri during the last six years.]. Turkiye Parazitol Derg. 2005;29(4):241-243.
pubmed - Noomene R, Ben Maamer A, Bouhafa A, Haoues N, Oueslati A, Cherif A. Primary hydatid cyst of the gallbladder: an unusual localization diagnosed by magnetic resonance imaging (MRI). Pan Afr Med J. 2013;14:15.
doi - Kapoor A, Sarma D, Gandhi D. Sonographic diagnosis of a ruptured primary hydatid cyst of the gallbladder. J Clin Ultrasound. 2000;28(1):51-52.
doi - Zangeneh M, Amerion M, Siadat SD, Alijani M. Primary hydatid cyst of the axillary region: a case report. Case Rep Med. 2012;2012:362610.
doi
This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.