

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 7, Number 11, November 2016, pages 498-501
A Rare but Lethal Malignant Cardiac Mass
Michael Cruz Caliza, d, Ivan Gonzalez-Cancelb, Ricardo Fernandeza, Modesto Gonzalezc, Gustavo Gonzaleza, Kelvin Rivera-Manzanoa
aPulmonary Department, San Juan City Hospital, San Juan, Puerto Rico
bCardiothoracic Surgery Department, Centro Cardiovascular de Puerto Rico y del Caribe, San Juan, Puerto Rico
cPulmonary Department, Centro Cardiovascular de Puerto Rico y del Caribe, San Juan, Puerto Rico
dCorresponding Author: Michael Cruz Caliz, Pulmonary Department, San Juan City Hospital, San Juan, Puerto Rico
Manuscript accepted for publication September 28, 2016
Short title: Lethal Malignant Cardiac Mass
doi: http://dx.doi.org/10.14740/jmc2663w
| Abstract | ▴Top |
Primary cardiac tumors are extremely rare. Incidence is approximately 0.017% of all primary tumors. Spindle cell sarcoma is the rarest, with only four cases reported and there are no guidelines for treating this condition. Cardiac sarcomas have symptoms by different mechanisms including obstruction, local invasion, and embolisms and in some cases the first manifestation could be a sudden cardiac death. Diagnosis is made with imaging techniques such as echocardiogram, cardiac computed tomography (CT), and magnetic resonance imaging (MRI) and confirmed with tissue biopsy. Patients with malignant tumors have a poor prognosis with an average mean survival of 6 months. Complete resection of the tumor remains the best treatment available. Spindle cell sarcoma may present with few symptoms and may remain silent until an advanced stage, thus limiting the few therapeutic options available.
Keywords: Cardiac tumor; Spindle cell sarcoma; Cardiac sarcoma; Cardiac mass
| Introduction | ▴Top |
Primary cardiac tumors both malignant and benign are extremely rare, even on specialized cardiothoracic surgery centers [1]. Cardiac tumors due to metastasis are 20 - 40 times more common than primary cardiac neoplasm [2]. The incidence reported in the literature is approximately 0.017-0.019% [3]. Of all primary cardiac tumors, 25% are malignant, of which 95% are sarcomas [4]. Spindle cell sarcoma is the least reported malignant tumor, with only four cases described in the literature [4-7]. Usually benign tumors have a good prognosis with normal life expectancy after complete surgical resection. However, patients with malignant tumors such as sarcomas have a poor prognosis even after a surgical intervention with an average mean survival of 6 months from the time of diagnosis [8].
| Case Report | ▴Top |
The patient was a 67-year-old Hispanic woman with a past medical history significant for arterial hypertension, dyslipidemia and diabetes mellitus type 2 without history of cardiac disease. Patient denied tobacco or alcohol habits. She presented to the emergency department with complaints of facial swelling and facial redness that was intermittent in nature for 1 year duration which was treated as an allergic reaction without improvement. Associated to original complaints, patient also reported unintentional weight loss of approximately 25 pounds during the previous 8 months, progressive shortness of breath and dry cough for the previous 2 months prior to arrival.
Physical examination findings were remarkable for bilateral jugular vein distention and facial swelling. Electrocardiogram (EKG) was remarkable for a normal sinus rhythm, and there was no evidence of ischemia with low voltage criteria (Fig. 1). Chest X-ray was remarkable for a round opacity of 3.8 × 3.7 cm at the right hilar region (Fig. 2). Further evaluation with chest computed tomography (CT) scan demonstrated a well-defined mass measuring 7 × 5.7 cm in the right atrium producing extrinsic compression and infiltration into the right atrioventricular valve and the proximal aspect of the right ventricle (Fig. 3). The mass infiltrated the right hilar region invading the pericardial fat (Fig. 3). In addition, the mass was producing a complete obliteration of the superior vena cava (SVC) (Fig. 3). Laboratories were remarkable for mild leukocytosis and cardiac enzymes were within normal limits. Echocardiogram was remarkable for an ejection fraction (EF) of 50-55%, mild enlargement of right and left ventricle, dilated inferior vena cava (IVC) and increased “echo signals” from the right atrium due to a mass effect. In view of previous findings, a myocardial biopsy was performed which yielded a positive result for a spindle cell sarcoma.
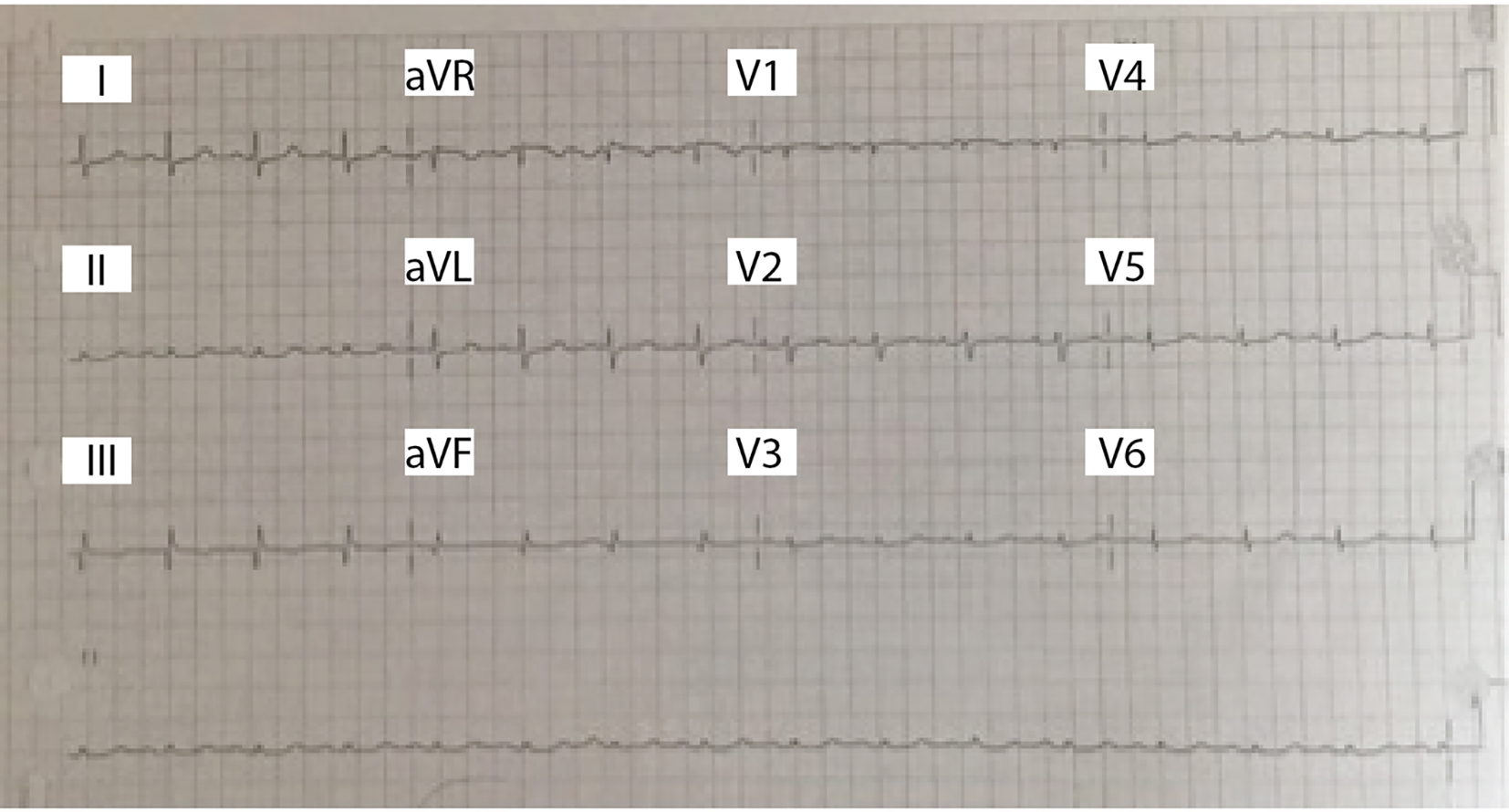 Click for large image | Figure 1. EKG with normal sinus rhythm, normal axis, no ST or ischemic changes, low voltage criteria present. |
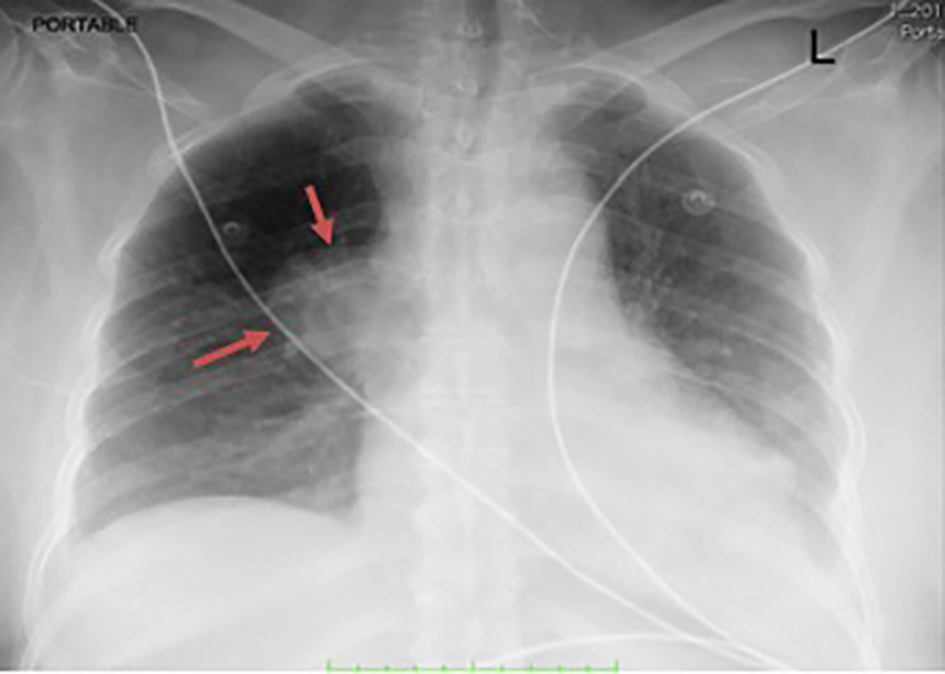 Click for large image | Figure 2. Chest X-ray. Orange arrows show 3.8 × 3.7 cm rounded radiopacity in the right hilar region. |
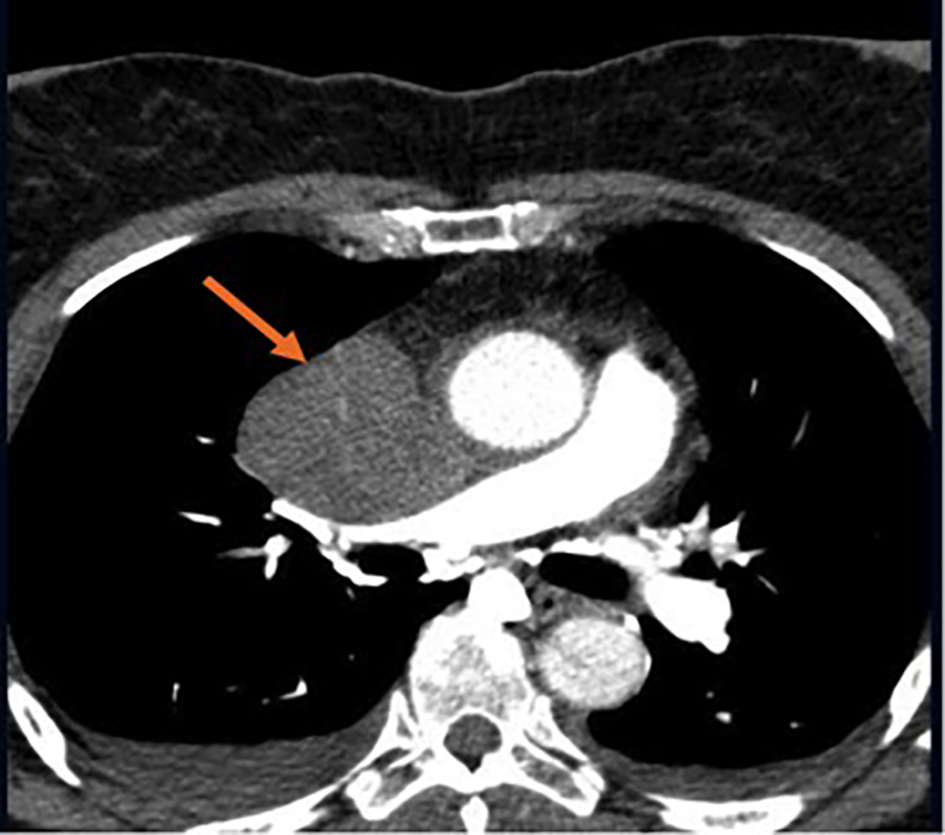 Click for large image | Figure 3. Chest CT scan. Orange arrow shows large mass measuring 7 × 5.7 cm in the right atrium producing extrinsic compression and infiltration into the right atrioventricular valve and the proximal aspect of the right ventricle. Extrinsic compression into the SVC with complete obliteration. |
After proper evaluation of the imaging studies, several surgical options were considered. Those options were: 1) conventional resection under cardiopulmonary bypass that may include resection of the total right atrium with tissue homograft or prosthetic reconstruction; 2) excision of the heart under cardiopulmonary bypass, ex vivo excision of the tumor and autotransplantation; and 3) total heart transplantation. These options, after a lengthy and detailed discussion with the patient, were all rejected for several anatomical and medical considerations. There are only very few reports in the literature that can sustain these approaches, all with dismay results. Moreover, on this patient, the tumor reaches beyond the confines of the SVC - in the case of the SVC, both the SVC and the innominate vein were thrombosed - and in relation to the IVC, the tumor reaches to the limit of the IVC - atrial junction. Due to the aggressive nature of these tumors, heart transplantation and immunosuppression were not considered feasible. Accordingly, the patient was referred to a specialized center where we believe a combined approach of chemoradiation may make the lesion surgically treatable but unfortunately, patient perished before starting therapy.
| Discussion | ▴Top |
The first case report of a cardiac tumor dated back to 1562, but Barnes et al described the first ante mortem diagnosis in 1934 through a biopsy [9-11]. The first successful surgery removing a primary cardiac tumor was reported in 1952 [12]. Since then, there have been cases of malignant tumors but nevertheless the management of these patients is not well defined and there are no evidence-based guidelines. Most of the data come from experience with few cases reported. The most common malignant tumor is the angiosarcoma [13]. The biopsy performed on our patient was positive for spindle cell sarcoma of the right atrium. This type of undifferentiated sarcoma is rare, with only four cases reported in the literature, which usually affects the left atrium, can infiltrate the pericardium and has a mesenchymal origin [3]. The spindle cell sarcoma is a highly aggressive tumor that metastized quickly and patients have a poor prognosis with a median survival of only 3 months to a year [3].
Cardiac sarcomas have symptoms by different mechanisms including obstruction, local invasion, and embolisms and in some cases the first manifestation could be a sudden cardiac death [1, 14]. Tumors located in the atrium or in the atrioventricular valves restrict blood and present with symptoms of cardiac failure [1]. Also if there is extension into the vena cava, an SVC syndrome can occur as in our patient [1]. Infiltration of the heart wall may occur as a restrictive or hypertrophic cardiomyopathy [1]. Thirty to 40% of patients may present an embolic event [15]. Up to 20% can cause cerebral ischemic stroke by cardiogenic embolism [15]. Other less specific symptoms are weight loss, fever, chest discomfort and syncope [14].
The diagnosis of primary cardiac tumors depends on the use of multiple modes of imaging techniques, including 2D echocardiogram, cardiac CT and cardiovascular magnetic resonance imaging (MRI) [16].
2D transthoracic echocardiography is the first modality for the screening and diagnosis of a cardiac tumor [14]. The sensitivity of 2D transthoracic echocardiogram is 93.3% [14]. Unlike echocardiogram, cardiac CT and cardiac MRI (CMRI) allow evaluation of additional major cardiac involvement and identify the presence of metastasis and infiltration [3]. MRI has the advantage over CT to evaluate the myocardium and pericardial involvement [14]. It also surpasses CT in the evaluation of tumor mass volume and tumor response to chemotherapy or surgery [3]. Despite the imaging technology available, definitive diagnosis of cardiac tumor is made through a tissue biopsy [2]. The biopsy may be percutaneous or transvenous, through endoscopy, mediastinoscopy or thoracotomy [2]. This allows us to evaluate the histology and malignant potential, which is important to establish a proper treatment and prognosis.
Whenever possible, a complete surgical resection in combination with chemotherapy is still the best treatment for primary cardiac tumors because the survival rate of these patients doubles [4]. However, both adjuvant chemotherapy and radiotherapy have not been very effective in the treatment of cardiac sarcomas [3]. Although it is known that the resection with negative borders is the best option, it is unfortunately plausible in less than 50% of cases [4]. Incomplete resection of the tumor in most cases results in recurrence [14].
There are different types of surgery in terms of primary cardiac tumors. Regarding malignant tumors, complex resection can be performed when the tumor is confined to heart and has not infiltrated other adjacent tissues [1]. Other techniques are “Ex situ resection” or “auto-transplantation” when the tumor involves the posterior wall of the left atrium or dorsal great vessels [1, 14]. With this surgical method, the heart is extracted outside the body for better anatomical visualization and re-implanted after tumor resection in the heart is repaired [1, 14]. Heart transplantation is an option for patients with inoperable sarcomas as an alternative therapy in case of no evidence of metastasis [2]. However, it is associated with recurrence of malignancy and new tumors stimulated by immunosuppression [14].
The prognosis of cardiac primary tumors, especially spindle cell sarcoma, is poor [4]. At the time of diagnosis, up to 80% of spindle cell sarcomas have evidence of metastasis, which worsens their prognosis [3]. These tumors may have few symptoms and remain silent until they reach an advanced stage, thus limiting the therapeutic options available. To the best of our knowledge, only four reported cases exist in the literature and there are no guidelines for treating this condition. It is recommended that once the diagnosis is made, these patients should be transferred to a specialized center for an early and aggressive treatment.
Acknowledgments
The authors would like to express their gratitude to Patricia Gonzalez BS, MBA, for the time and effort it took to correct and edit our work. We were able to do this work better with your help and knowledge.
Funding
This case report did not receive any specific grant from any funding agency in the public, commercial or non-profit sector.
Conflicts of Interest
There are no conflicts of interest that could be perceived as prejudicing the impartiality of this case.
| References | ▴Top |
- Hoffmeier A, Sindermann JR, Scheld HH, Martens S. Cardiac tumors - diagnosis and surgical treatment. Dtsch Arztebl Int. 2014;111(12):205-211.
pubmed - Mehta N, Desai A, Shivdasani B, Suryawanshi S, Mehta AB, Behranwala A, Dhabhar B. Left atrial spindle cell sarcoma - case report. Indian Heart J. 2012;64(4):416-419.
doi pubmed - Muturi A, Kotecha V, Ruturi J, Muhinga M, Waweru W. High-grade spindle cell sarcoma of the heart: a case report and review of literature. J Cardiothorac Surg. 2015;10:46.
doi pubmed - Ibrahim A, Luk A, Singhal P, Wan B, Zavodni A, Cusimano RJ, Butany J. Primary intimal (spindle cell) sarcoma of the heart: a case report and review of the literature. Case Rep Med. 2013;2013:461815.
doi - Li Z, Hsieh T, Salehi A. Recurrent cardiac intimal (spindle cell) sarcoma of the left atrium. J Cardiothorac Vasc Anesth. 2013;27(1):103-107.
doi pubmed - Cho GJ, Kim HJ, Kang JS. Primary cardiac sarcoma in pregnancy: a case report. J Korean Med Sci. 2006;21(5):940-943.
doi pubmed - Modi A, Lipnevicius A, Moorjani N, Haw M. Prolonged survival with left atrial spindle cell sarcoma. Interact Cardiovasc Thorac Surg. 2009;8(6):703-704.
doi pubmed - Elbardissi AW, Dearani JA, Daly RC, Mullany CJ, Orszulak TA, Puga FJ, Schaff HV. Survival after resection of primary cardiac tumors: a 48-year experience. Circulation. 2008;118(14 Suppl):S7-15.
doi pubmed - Simpson L, Kumar S, Okuno S, Schaff H, Porrata L, Buckner J, Moynihan T. American Cancer Society 2008. www.interscience.wiley.com.
doi - Colombus MR. De Re Anatomica. Paris:1562:482.
- Barnes AR, Beaver DC, Snell AM. Primary sarcoma of heart: report of a case with electrocardiographic and pathological studies. Am Heart J. 1934;9:480.
doi - Maurer ER. Successful removal of tumor of the heart. J Thorac Surg. 1952;23(5):479-485.
pubmed - Mehra S, Ibrahim O, Moshiri M, Cahill J, Bhargava P. Spindle-cell sarcoma of the hear: A rare cause for cardiac mass. Radiology case reports. 2012.
doi - Shanmugam G. Primary cardiac sarcoma. Eur J Cardiothorac Surg. 2006;29(6):925-932.
doi pubmed - Jassal DS, Thakrar A, Neilan TG, Isselbacher EM, Brugge WR, King ME. Cardioembolic stroke in a patient with spindle cell sarcoma of the left atrium. J Am Soc Echocardiogr. 2007;20(4):438 e431-434.
- Leja MJ, Shah DJ, Reardon MJ. Primary cardiac tumors. Tex Heart Inst J. 2011;38(3):261-262.
pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.