

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 7, Number 12, December 2016, pages 536-538
Adenocystic Carcinoma of the External Auditory Canal: A Case Report and Review of the Literature
Pinelopi Theopisti Memtsaa, c, Aikaterini Papadopouloub, Konstantina Bonioua, Panagiotis Diafasa, Ioannis Tzitzikasb, Martha Charalambidoua
aDepartment of Radiation Oncology, Cancer Hospital of Thessaloniki Theageneio, Thessaloniki, Greece
bDepartment of Radiation Oncology, AHEPA Hospital, Aristotle University, Thessaloniki, Greece
cCorresponding Author: Pinelopi Theopisti Memtsa, Department of Radiation Oncology, Cancer Hospital of Thessaloniki Theageneio, Psarron 26, 54453 Thessaloniki, Greece
Manuscript accepted for publication November 09, 2016
Short title: Adenocystic Carcinoma of External Auditory Canal
doi: https://doi.org/10.14740/jmc2689w
| Abstract | ▴Top |
Primary external auditory canal (EAC) malignancies are very rare with adenoid cystic carcinoma (ACC) representing approximately 5% of these tumors. The majority of these patients present with constant ear pain of prolonged duration, hearing loss and a mass in the external ear canal. The treatment is surgical resection and postoperative radiation therapy. However, the overall prognosis is poor due to recurrences and distant metastasis. In this article, we report a case of ACC of the EAC with a review of the literature.
Keywords: External auditory canal; Radiation therapy; Adenocystic carcinoma
| Introduction | ▴Top |
Primary cancers of the external auditory canal (EAC) are rare and most are squamous cell carcinoma. Those of glandular origin comprise just 20% of EAC tumors, with adenoid cystic carcinoma (ACC) of EAC being extremely rare [1]. Adenocystic carcinoma of the head and neck is usually found in the salivary glands, oral cavity, nasopharynx, and palate [2]. There have been only a few cases of adenocystic carcinoma involving the EAC reported in the international literature. An adolescent clinical course which usually leads to a late diagnosis is the main characteristic of the adenocystic carcinoma of the EAC [3]. The mainstay of treatment is the surgical excision with main goal of the achievement of clear margins because of the high risk of repeat local recurrence [4].
Due to the rarity of the adenocystic carcinoma of the EAC, there are very little evidence about long-term outcome and follow-up.
In this article, we present a case of ACC of the EAC along with a review and discussion of the literature to date.
| Case Report | ▴Top |
A 56-year-old woman was admitted to our hospital with otalgia since 2008, which was treated with conservative treatment with analgesics and antibiotics. In 2012, the patient underwent a computed tomography (CT) scan of the visceral skull, which revealed a well circumscribed mass of 6.6 mm maximum diameter which was directly in contact with the cartilaginous part of the ear canal without any signs of invasion. The patient underwent surgical removal of the lesion. The histological report confirmed the diagnosis of an intermediate grade (grade II) ACC of the EAC with perineural invasion. The tumor was composed of basaloid cells and few areas of necrosis were noted. The immunohistochemistry results were positive for CK8/18, EMA, SMA, CD117/cKit and S100. Ki67 labeling index was 30% (Figs. 1 and 2). The invaded deep surgical margin was the reason for the second operation to ensure clear resection margins. A month later, the patient underwent a surgical removal of the superficial lobe of the parotid gland and ipsilateral cervical dissection. The histology was negative for malignancy. Two months after surgery, she attended our department for postoperative irradiation. The radiotherapy was performed in a linear accelerator with 6-MV energy, with a three-dimensional conformal radiation delivery technique. She received a total dose of 50 Gy in 25 fractions with a daily dose of 2 Gy in the tumor bed and a total dose of 44 Gy in the ipsilateral cervical lymph nodes. The patient was followed up at 3 monthly intervals with clinical examination and CT in the first year and then twice yearly. The patient has no evidence of disease recurrence during 41 months of follow-up.
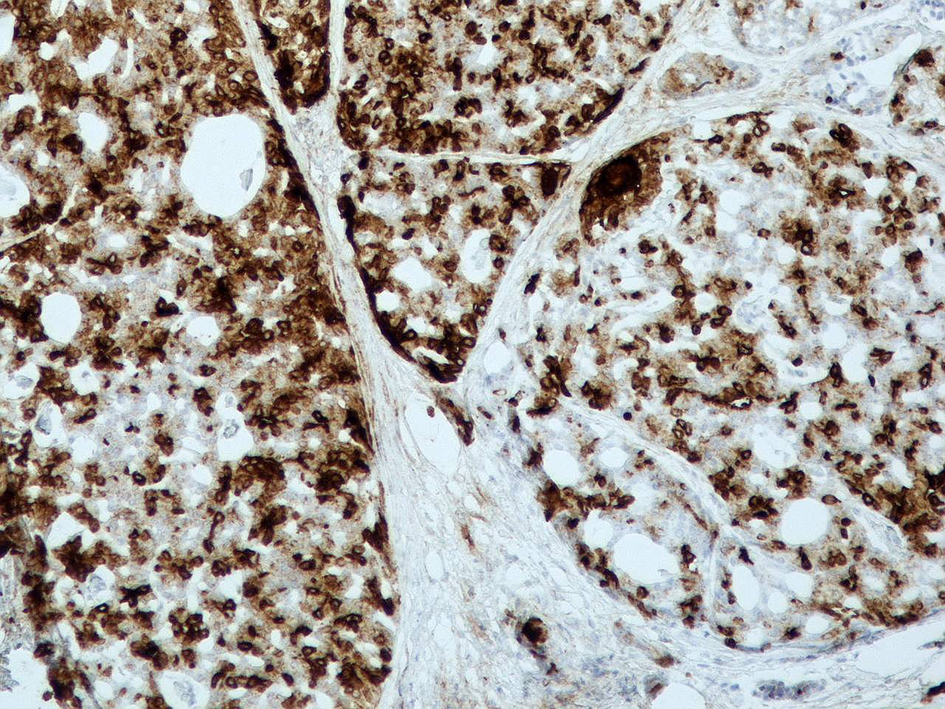 Click for large image | Figure 1. An image from the immunochemistry of the CK8/18. |
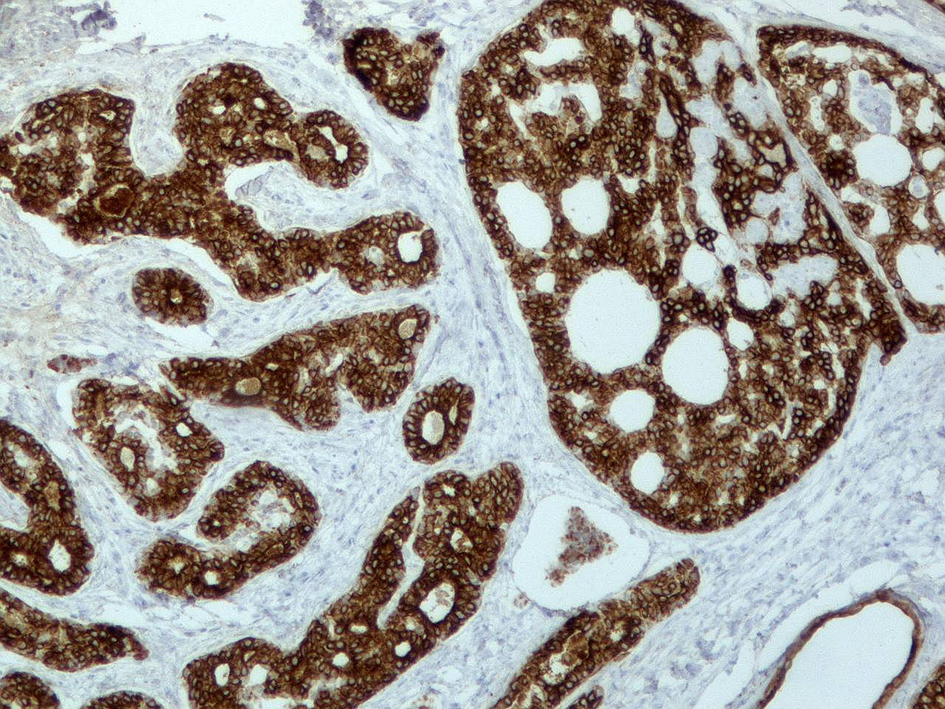 Click for large image | Figure 2. An image from the immunochemistry of epithelial membrane antigen. |
| Discussion | ▴Top |
Adenocystic carcinoma of the EAC is extremely rare, approximately 5%, therefore it is very rarely encountered in the everyday clinical practice. The mean age for ACC is the fifth decade and it is two times more common in women than men. The most common clinical symptoms are otorrhea, pain, hearing loss, bleeding and a mass in the ear canal [5]. A wide deep biopsy should be performed in every EAC mass, as it is essential for the establishment of the diagnosis of adenocystic carcinoma. The use of MRI in these cases has not been fully delineated. Gadolinium-DTPA contrast-enhanced MRI is most helpful in demonstrating infiltration into surrounding tissues [6].
The true origin of adenocystic carcinoma of the EAC has not yet been defined, yet it is proposed that these tumors may arise from ectopic salivary glands. Three main histologic patterns of ACC have been described: tubular, cribriform and solid [7]. The tubular pattern seems to have the best prognosis; however, the relationship between histopathology and prognosis remains unclear because of the limited number of cases and inadequate long-term follow-up. Adenocystic carcinoma of the EAC is more aggressive than adenocystic carcinoma arising in the salivary glands and leads to poor prognosis [8].
Adenocystic carcinoma has a high propensity towards perineural involvement, which explains why one of the most common symptoms is otalgia. When perineural and lymphovascular invasion is present, the tumor recurrence rate is higher [9, 10].
The treatment of adenocystic carcinoma of the EAC depends on complete surgical resection with clear margins. Other important prognostic factors are the involvement of the parotid gland, nerve and bone. For that reason, elective parotidectomy is recommended [11].
It is difficult to determine the role of postoperative radiation therapy in adenocystic carcinoma of the EAC, due to the limited number of patients. However, it is suggested when positive microscopic margins are present, in advanced T stage, in cervical nodal metastasis, in solid histologic pattern, in perineural invasion and in recurrent tumors [12].
In spite of aggressive and early management, patients with adenocystic carcinoma of the EAC often experience recurrences. Metastasis to regional lymph nodes and distant sites, like lungs, are very common [13].
Conclusion
Adenocystic carcinoma is a rare neoplasm originating in the EAC. Patients with long-standing otalgia and ear canal mass should be considered for biopsy and imaging. Early aggressive surgical management with adjuvant radiotherapy may help to prevent distant metastasis [14]. More multicenter randomized trials with long-term follow-up should be performed so as to have evidence about the sequence of the treatments and the role of radiotherapy and chemotherapy in these neoplasms.
| References | ▴Top |
- Gidley PW. Managing malignancies of the external auditory canal. Expert Rev Anticancer Ther. 2009;9(9):1277-1282.
doi pubmed - Dong F, Gidley PW, Ho T, Luna MA, Ginsberg LE, Sturgis EM. Adenoid cystic carcinoma of the external auditory canal. Laryngoscope. 2008;118(9):1591-1596.
doi pubmed - Sigal R, Monnet O, de Baere T, Micheau C, Shapeero LG, Julieron M, Bosq J, et al. Adenoid cystic carcinoma of the head and neck: evaluation with MR imaging and clinical-pathologic correlation in 27 patients. Radiology. 1992;184(1):95-101.
doi pubmed - Nayak SP, Walke VA, Helwatkar SB, Bobhate SK. Adenoid cystic carcinoma of the external auditory canal: report of two cases. Indian J Pathol Microbiol. 2009;52(4):540-542.
doi pubmed - Liu SC, Kang BH, Nieh S, Chang JL, Wang CH. Adenoid cystic carcinoma of the external auditory canal. J Chin Med Assoc. 2012;75(6):296-300.
doi pubmed - Aikawa H, Tomonari K, Okino Y, Hori F, Ueyama T, Suenaga S, Bundo J, et al. Adenoid cystic carcinoma of the external auditory canal: correlation between histological features and MRI appearances. Br J Radiol. 1997;70(833):530-532.
doi pubmed - Perzin KH, Gullane P, Conley J. Adenoid cystic carcinoma involving the external auditory canal. A clinicopathologic study of 16 cases. Cancer. 1982;50(12):2873-2883.
doi - Perzin KH, Gullane P, Clairmont AC. Adenoid cystic carcinomas arising in salivary glands: a correlation of histologic features and clinical course. Cancer. 1978;42(1):265-282.
doi - Garbyal RS, Kumar M, Bohra A. Adenoid cystic carcinoma of ceruminous gland: a case report. Indian J Pathol Microbiol. 2006;49(4):587-589.
pubmed - Shang J, Sheng L, Wang K, Shui Y, Wei Q. Expression of neural cell adhesion molecule in salivary adenoid cystic carcinoma and its correlation with perineural invasion. Oncol Rep. 2007;18(6):1413-1416.
doi - Chang CH, Shu MT, Lee JC, Leu YS, Chen YC, Lee KS. Treatments and outcomes of malignant tumors of external auditory canal. Am J Otolaryngol. 2009;30(1):44-48.
doi pubmed - Silverman DA, Carlson TP, Khuntia D, Bergstrom RT, Saxton J, Esclamado RM. Role for postoperative radiation therapy in adenoid cystic carcinoma of the head and neck. Laryngoscope. 2004;114(7):1194-1199.
doi pubmed - Koopot R, Reyes C, Pifarre R. Multiple pulmonary metastases from adenoid cystic carcinoma of ceruminous glands of external auditory canal. A case report and review of the literature. J Thorac Cardiovasc Surg. 1973;65(6):909-913.
pubmed - Prokopakis EP, Snyderman CH, Hanna EY, Carrau RL, Johnson JT, D'Amico F. Risk factors for local recurrence of adenoid cystic carcinoma: the role of postoperative radiation therapy. Am J Otolaryngol. 1999;20(5):281-286.
doi
This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.