

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 2, Number 4, August 2011, pages 166-168
Single Coronary Artery With Anomalous Origin From the Right Sinus Valsalva: A Rarity in the Catheterization Laboratory
Davran Ciceka, d, Yavuz Ulucab, Haldun Muderrisogluc
aDepartment of Cardiology, Baskent University School of Medicine, Saray Mah, Yunusemre cad, No: 1 07400, Antalya, Turkey
bDepartment of Cardiology, Bayindir Hospital, Istanbul, Turkey
cDepartment of Cardiology, Baskent University School of Medicine, Bahcelievler, No: 1, Ankara, Turkey
dCorresponding author: Davran Cicek, Department of Cardiology, Baskent University School of Medicine, Saray Mah, Yunusemre cad, No: 1 07400, Antalya, Turkey
Manuscript accepted for publication May 20, 2011
Short title: Single Coronary Artery
doi: https://doi.org/10.4021/jmc239e
| Abstract | ▴Top |
A single coronary artery is a rare congenital anomaly with an incidence of 0.02%. We report a 74-year-old Caucasian female presenting with angina pectoris, effort dyspnea and a history of hypertension and hypercholesterolemia, being diagnosed with a very rare variant of a single coronary artery arising from the right sinus of Valsalva continuing as right coronary artery (RCA) and thereafter as left anterior descending coronary artery (LAD). Because the patient was asymptomatic with ischemic medication and had a proposed relative benign course, we recommended medical treatment without coronary artery bypass surgery. Twelve months after angiography the patient has been in fine condition and asymptomatic under medical treatment. Cardiologist should keep in mind that patients with coronary artery anomalies are usually asymptomatic. They may develop clinical symptoms like syncope, angina pectoris, ventricular arrhythmias, myocardial infarction and sudden death. The treatment strategy for single coronary artery is still not clear.
Keywords: Coronary anomalies; Single coronary artery (SCA)
| Introduction | ▴Top |
Anomalous origin of the coronary arteries is an infrequent congenital abnormality, and has been found in about 1% of adult patients undergoing coronary angiography [1-3]. Single coronary artery arising from the right sinus of Valsalva is a rare congenital coronary anomaly, particularly in the absence of other cardiac congenital diseases. In fact, it is often associated with a bicuspid aortic valve, mitral valve prolapse and ventricular septal defect, and it is reported to constitute only 0.017% of angiographic series [1-6].
We present a case of a single coronary artery arising from the right aortic sinus, the presence of which was suspected following coronary angiography.
| Case Report | ▴Top |
We report a 74-year-old Caucasian female, with a 30-year history of hypertension treated with angiotensin-converting enzyme (ACE) inhibitor and diuretics. The patient was in atrial fibrillation with a heart rate of approximately 98 beats/min. On her electrocardiogram, there were negative T waves in leads V1 - V4. The patient was admitted to the coronary care unit for further evaluation. Cardiac biomarkers were not significant. Following medical treatment with aspirin, beta-blocker, statin, angiotensin-converting enzyme, and nitrate, her angina pectoris was resolved. Transthoracic echocardiography demonstrated hypokinesia of the inferior wall of the left ventricle. Ejection fraction was estimated as 44% by the modified Simpson’s method. Coronary angiography was performed. The left coronary artery ostium could not be cannulated selectively (Fig. 1, 2). Selective cannulation of the right sinus of Valsalva demonstrated a single coronary artery originating from the right sinus of Valsalva, and giving off branches to the right coronary artery (RCA) and the left coronary system (Fig. 3). The single coronary artery was classified as type R-I. There were no significant stenotic lesions in the RCA and left anterior descending coronary artery (LAD). The patient underwent medical treatment. She remained free of angina pectoris within 12 months after coronary angiography.
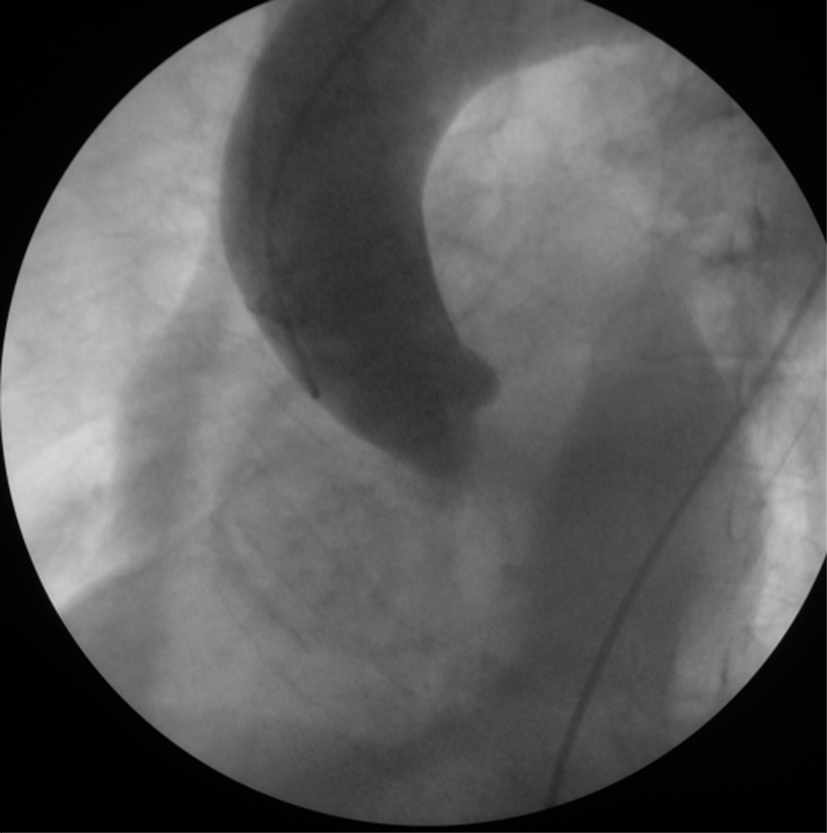 Click for large image | Figure 1. Aortography with pigtail catheter. There is no left coronaryartery in the aortography. |
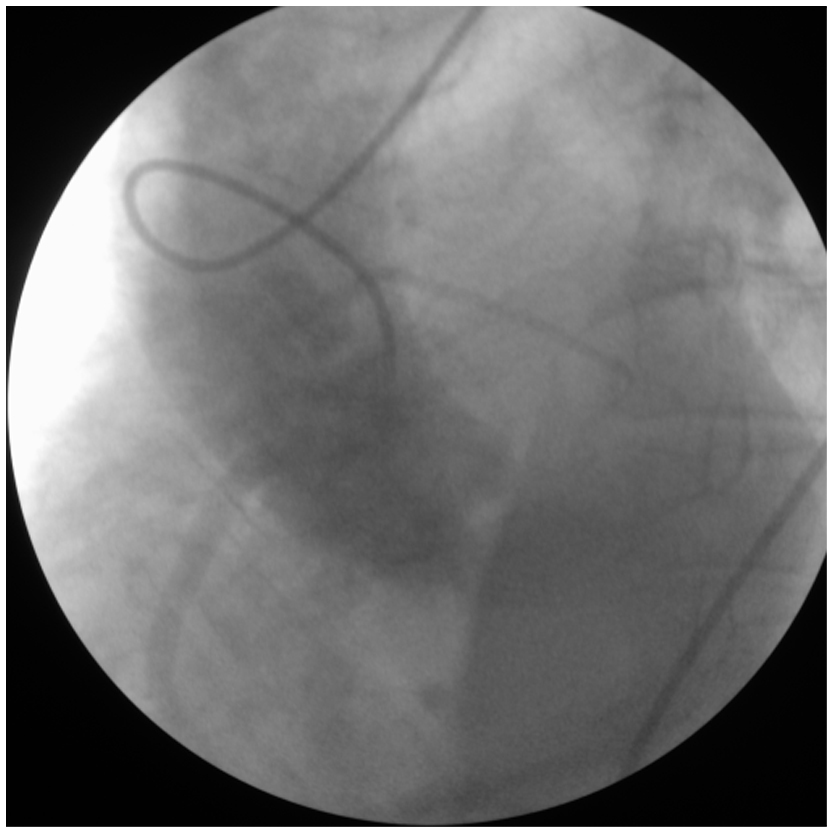 Click for large image | Figure 2. Non-selective injection to the aorta with sones catheter. |
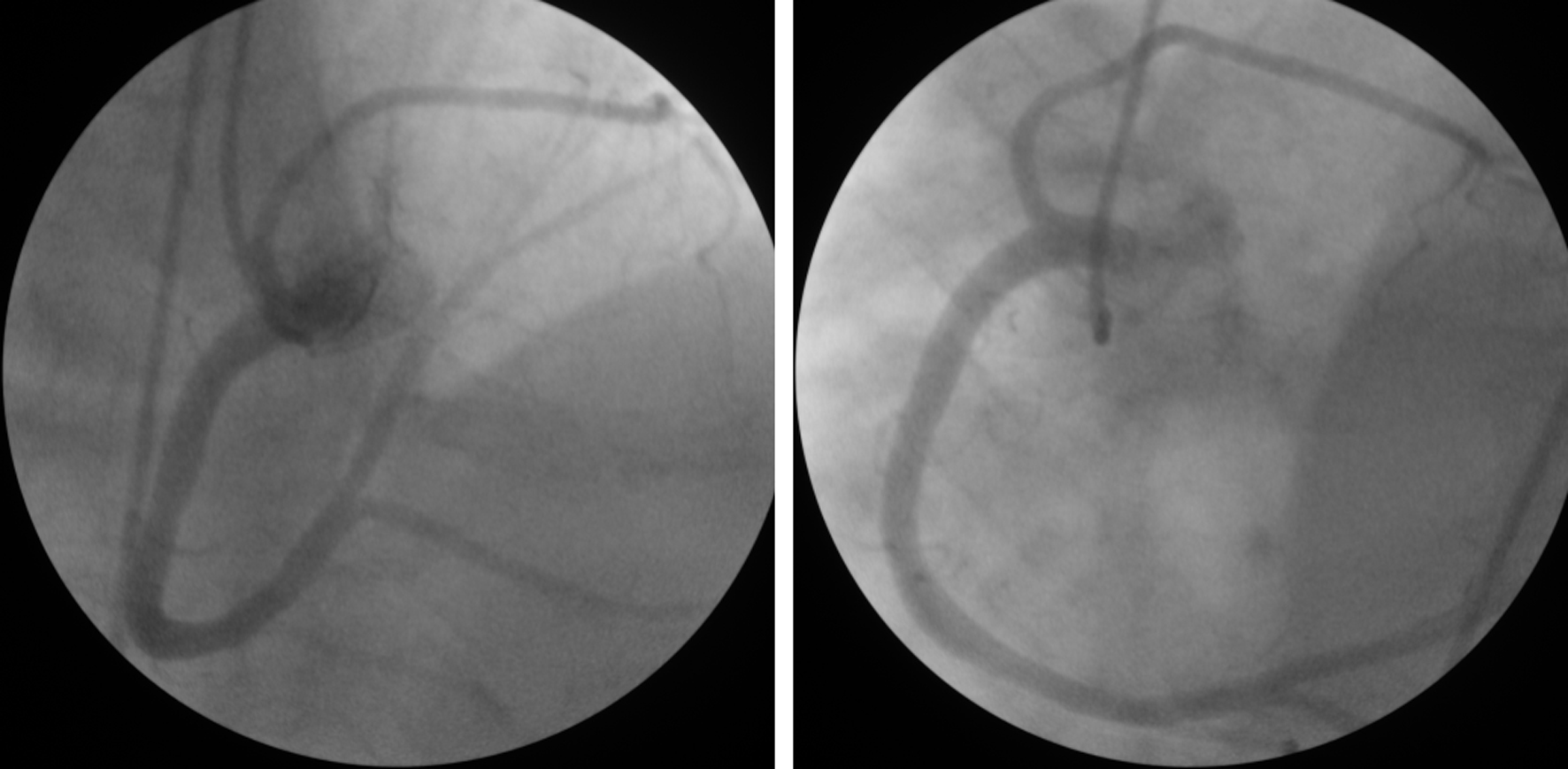 Click for large image | Figure 3. The single coronary artery originates from the right sinus of Valsalva and gives branches to the RCA and the left coronary system (type R-I). |
| Discussion | ▴Top |
Coronary anomalies are not recognized during routine screening. In general, they are diagnosed incidentally during conventional coronary angiography. In 1979, Lipton et al. proposed a very useful angiographic classification [7], later modified by Yamanaka and Hobbs [2] in 1990. This classification begins with a division into the “R” (right) and the “L” (left)-type, according to whether the single coronary artery (SCA) originates from the right or the left sinus of Valsalva. Thereafter, every case is designated as belonging to group I, II or III, depending on the anatomical course of the artery. In group I, the artery follows the anatomical course of either a right or a left coronary artery. In groups II and III, an important characteristic of this classification is the path followed by the anomalous arteries from one side of the heart to the other: “A” denotes a path anterior to the great vessels, while “P” denotes a posterior course; “B” indicates a path between the aorta and the pulmonary artery and “S” is used when part of the route is through the interventricular septum; finally, “C” stands for a combination of diverse routes. To improve communication and transmission of angiographic data, all coronary anomalies were categorized in a new angiographic classification proposed by Rigatelli et al. [8]. The SCA was angiographically classified by Rigatelli, following Lipton classification, as radical hyperdominance of a coronary artery that fills the entire coronary tree (class II). In our case, the SCA was included in the R-I group, in which a very large RCA continues in the atrioventricular groove, extending to the anterior base of the heart where it gives rise to an anterior descending branch.
Although patients with coronary artery anomalies are usually asymptomatic, they may develop clinical symptoms like syncope, angina pectoris, ventricular arrhythmias, myocardial infarction and sudden death without evidence of coronary atherosclerosis, depending on the type of coronary anomaly. In fact, anomalous origin of the coronary arteries has been reported as the cause of 5 - 35% of sudden cardiac death in young people especially during efforts, because of dilation of aortic root and pulmonary artery, which may cause compression of an abnormal coronary artery with retroaortic course [9, 10]. These anomalies have also been associated with myocardial ischemia and arrhythmias during exercise [10, 11].
Single coronary artery may be an asymptomatic congenital alteration detected in patients with myocardial ischemia due to atherosclerotic coronary artery disease. In these cases, percutaneous coronary angioplasty with stent insertion may be a successful therapeutic option; however, accurate morphologic identification of anomalous arteries is mandatory before planning these interventions, in order to recognize other possible mechanisms of myocardial ischemia (e.g., vascular compression) and to choose the most appropriate type of pharmacological, percutaneous or surgical intervention. Other imaging techniques, like coronary computed tomography or magnetic resonance imaging, may be useful in order to correctly identify the origin and course of abnormal coronary arteries.
In summary, the treatment strategy for single coronary artery is not clear. The course and associated coronary atherosclerosis should guide the therapy. Coronary artery bypass surgery may be beneficial in patients whose anomalous coronary artery courses between the aorta and main pulmonary artery or/and patients with atherosclerosis may benefit from revascularization strategies.
Authors’ Contributions
DC performed the coronary angiography and was a major contributor in writing the manuscript. DC, YU and HM worked together in writing the manuscript. All authors read and approved the final manuscript.
Competing Interests
The authors declare that they have no competing interests.
| References | ▴Top |
- Aydinlar A, Cicek D, Senturk T, Gemici K, Serdar OA, Kazazoglu AR, Kumbay E, et al. Primary congenital anomalies of the coronary arteries: a coronary arteriographic study in Western Turkey. Int Heart J 2005;46(1):97-103.
pubmed doi - Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn 1990;21(1):28-40.
pubmed doi - Garg N, Tewari S, Kapoor A, Gupta DK, Sinha N. Primary congenital anomalies of the coronary arteries: a coronary: arteriographic study. Int J Cardiol 2000;74(1):39-46.
pubmed doi - Angelini P. Coronary artery anomalies—current clinical issues: definitions, classification, incidence, clinical relevance, and treatment guidelines. Tex Heart Inst J 2002;29(4):271-278.
pubmed - Gowda RM, Chamakura SR, Dogan OM, Sacchi TJ, Khan IA. Origin of left main and right coronary arteries from right aortic sinus of Valsalva. Int J Cardiol 2003;92(2-3):305-306.
pubmed doi - Ozeren A, Aydin M, Bilge M, Cam F. Anomalous left coronary artery arising from the right sinus of Valsalva: a case report. Int J Cardiol 2005;101(3):491-493.
pubmed doi - Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology 1979;130(1):39-47.
pubmed - Rigatelli G, Docali G, Rossi P, Bovolon D, Rossi D, Bandello A, Lonardi G. Congenital coronary artery anomalies angiographic classification revisited. Int J Cardiovasc Imaging 2003;19(5):361-366.
pubmed doi - Maron BJ. Triggers for sudden cardiac death in the athlete. Cardiol Clin 1996;14(2):195-210.
pubmed - Basso C, Corrado D, Thiene G. Congenital coronary artery anomalies as an important cause of sudden death in the young. Cardiol Rev 2001;9(6):312-317.
pubmed doi - Iskandar EG, Thompson PD. Exercise-related sudden death due to an unusual coronary artery anomaly. Med Sci Sports Exerc 2004;36(2):180-182.
pubmed doi
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.