Gastric perforation from metastatic breast cancer is a rare complication that is difficult to treat. Herein, we report a case of an 81-year-old female patient with neglected invasive lobular breast cancer causing gastric perforation due to metastasis. She underwent palliative surgical intervention with partial gastric resection. After 6 months, she is doing well.
Keywords: Gastric perforation; Metastatic breast cancer; Invasive lobular cancer
Gastric metastases due to primary breast cancer are in general rare, although the stomach represents the most common site of metastatic lesions from breast cancer [1]. It more frequently metastasizes to the stomach lobular carcinoma than ductal. Symptoms of metastatic gastric cancer are similar to those of primary gastric cancer [2]. The differentiation between these two is essential regarding the treatment options. Therapy for metastatic gastric cancer is mainly systemic with chemotherapy and hormones, whereas surgical intervention is applied in limited occasions [3], such as gastric perforation. Perforated gastric cancer accounts for less than 1% [4, 5]. Resulting peritonitis is a life-threatening condition that mandates emergency laparotomy. Depending on the findings, surgical procedure varies from single closure with or without omental patch to gastric resection.
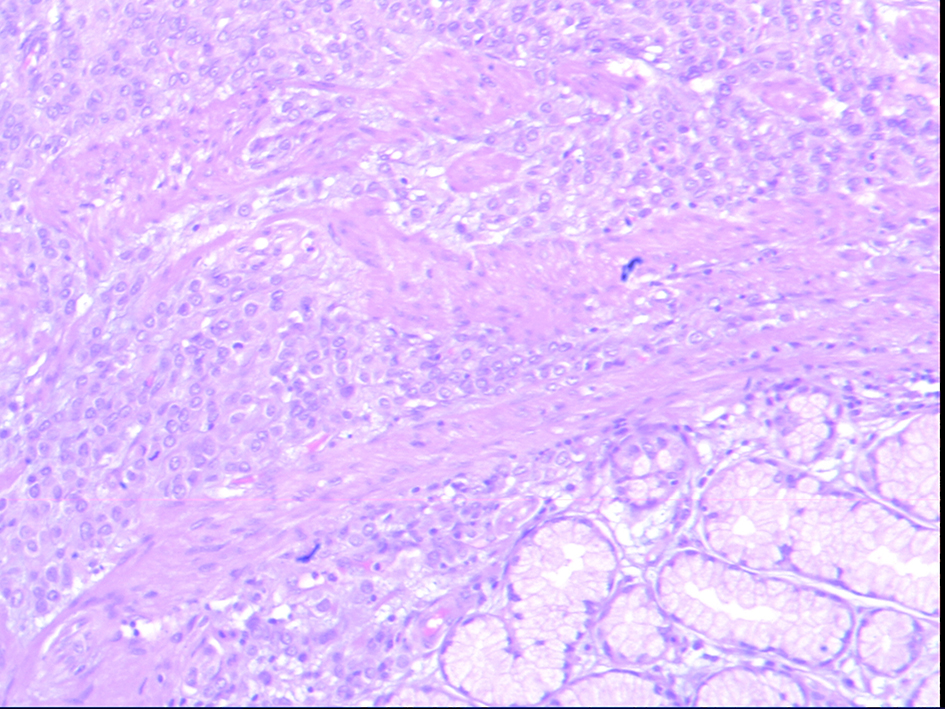
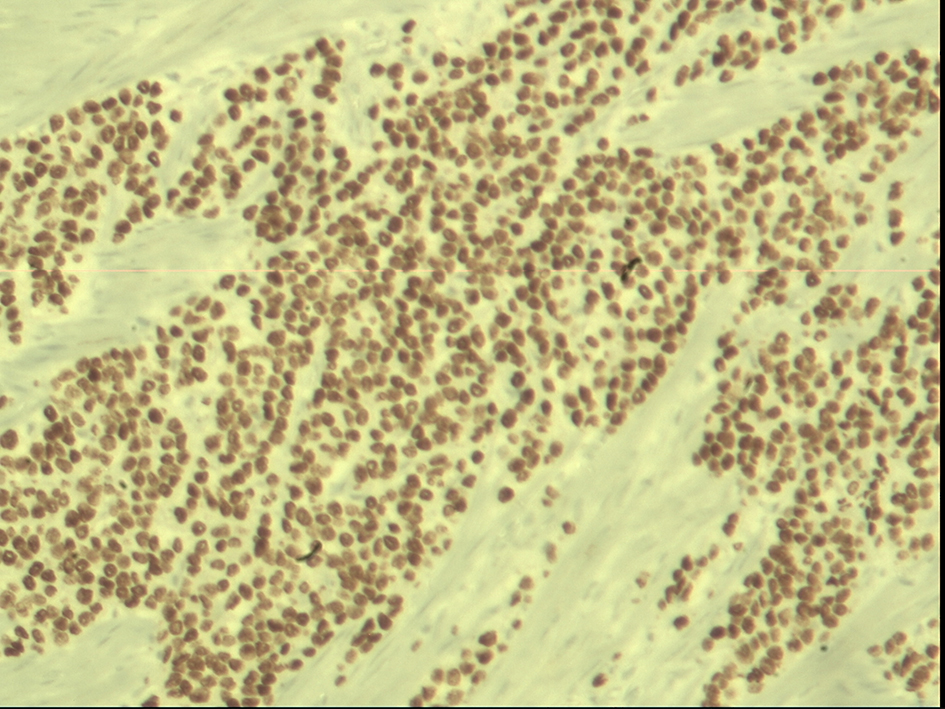
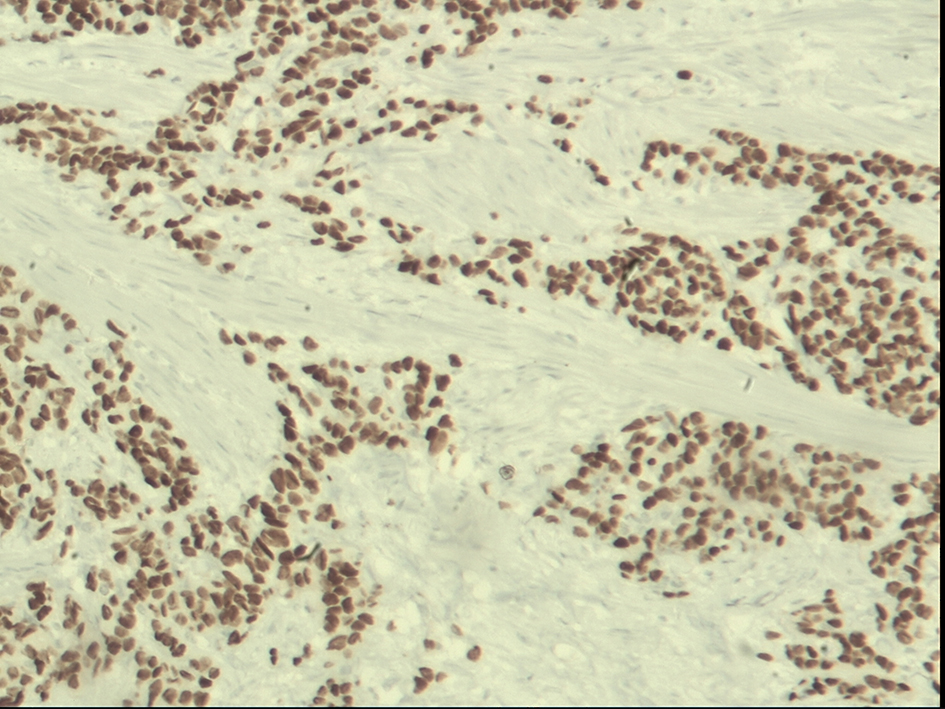
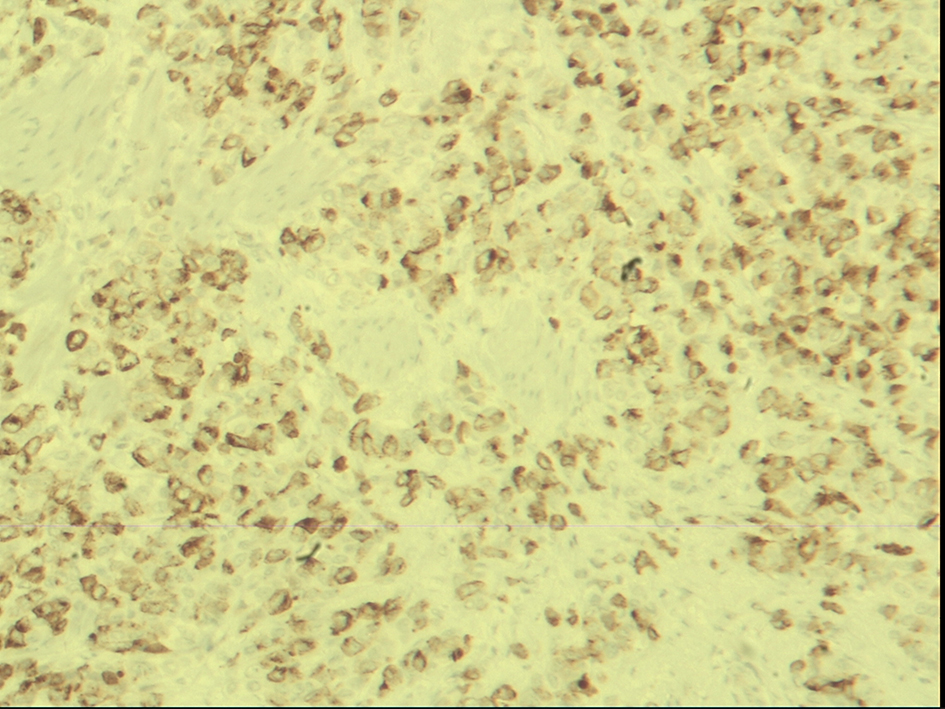
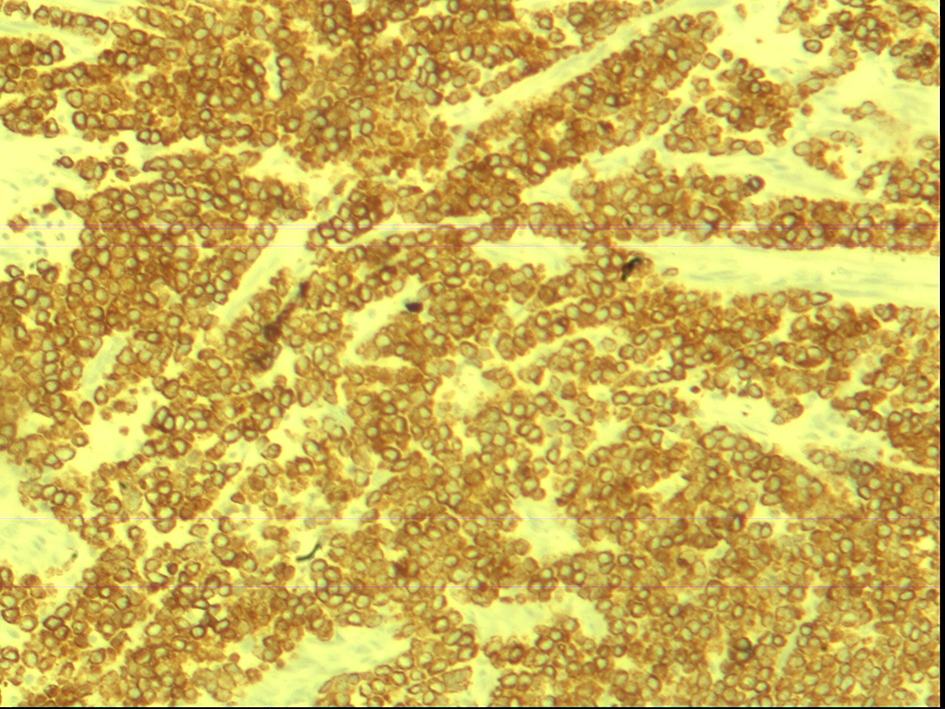
An 81-year-old female patient was admitted to the emergency department of our hospital suffering from epigastric pain and vomiting. From her medical history, she had a palpable mass of the left breast, for which she was aware but it was left untreated for 7 years. Five days before her admission, she had abdominal CT scan negative for free air or fluid collections. After being admitted to the internists for 1 day, she was referred to us for a surgical opinion. Clinical examination revealed abdominal tenderness. Conducted CT scan of the chest and the abdomen showed bilateral invasive breast cancer and pneumoperitoneum (Figs. 1 and 2). The patient underwent immediate exploratory laparotomy which revealed a large perforation of the stomach, 3 - 4 cm in greater diameter, located on the anterior wall of the antrum. In palpation, a solid mass occupying the antrum was noticed. A R1 antrectomy with Billroth II gastrointestinal reconstruction was performed. Histopathological examination of the specimen indicated extensive metastatic infiltration of the gastric wall, arising from malignant epithelial neoplasm with morphologic and immunohistochemical characteristics compatible with invasive breast cancer (most probably lobular) (Figs. 3-7). In particular, metastatic neoplasm invaded the serosa, muscularis and mucosal membrane of the gastric wall. The surgical margins were infiltrated from metastatic disease. Postoperative recovery lasted 2 weeks due to moderate respiratory complications that were treated successfully. The patient was referred to the oncologists for further treatment. Six months postoperatively, the patient is alive, under chemotherapeutic regimen and oncological consultation. Her general medical condition is good, without needing any reoperation.
The most frequent primary malignant lesion that metastasizes to the stomach is breast cancer, followed by renal cell cancer [6]. Invasive lobular breast cancer is the histological type that spreads to the gastrointestinal tract more often than invasive ductal [7, 8]. Usually, there is a dissemination of the disease at the time of diagnosis of gastric metastasis from breast cancer [8, 9]. Moreover, in cases of perforated gastric cancer, there is peritoneal contamination additionally to the advanced malignancy. Therefore, the poor general condition of the patient is a limitation for curative surgical resection, in form of total or subtotal gastrectomy, which would offer much better prognosis and survival rate of the patient [5]. Unfortunately, gastric resection can be performed in selected cases only. In most cases of gastric perforation from metastatic cancer, simple closure with omental patch is applied, although a high rate of reperforation occurs. In our case, the defect at the stomach was large enough to be closed by simple suture or omental patch. The patient was stable enough and tolerated a quickly performed partial resection of the stomach.
As gastric perforation with resulting peritonitis represents a life-threatening condition that needs immediate surgical intervention, the choice of the best applied procedure should be based on every time patient’s comorbidity and hemodynamic status as well as on surgical findings and expertise.
Namikawa T, Hanazaki K. Clinicopathological features and treatment outcomes of metastatic tumors in the stomach. Surg Today. 2014;44(8):1392-1399. doipubmed
Pectasides D, Psyrri A, Pliarchopoulou K, Floros T, Papaxoinis G, Skondra M, Papatsibas G, et al. Gastric metastases originating from breast cancer: report of 8 cases and review of the literature. Anticancer Res. 2009;29(11):4759-4763. pubmed
Jones GE, Strauss DC, Forshaw MJ, Deere H, Mahedeva U, Mason RC. Breast cancer metastasis to the stomach may mimic primary gastric cancer: report of two cases and review of literature. World J Surg Oncol. 2007;5:75. doipubmed
Serban D, Branescu C, Savlovschi C, El-Khatib A, Tudor C, Nica A, Kraft A, et al. Complex histopathological and surgical aspects in a case of giant malignant gastric perforation. J Med Life. 2016;9(2):216-219. pubmed
Ignjatovic N, Stojanov D, Djordjevic M, Ignjatovic J, Benedeto Stojanov D, Milojkovic B. Perforation of gastric cancer - What should the surgeon do? Bosn J Basic Med Sci. 2016;16(3):222-226. doi
Weigt J, Malfertheiner P. Metastatic Disease in the Stomach. Gastrointest Tumors. 2015;2(2):61-64. doipubmed
Rachan Shetty KS, Challa VR, Lakshmaiah KC, Champaka G, Babu KG. Gastric metastases from breast cancer: A report of two cases and review of literature. J Cancer Res Ther. 2015;11(3):660. doipubmed
McLemore EC, Pockaj BA, Reynolds C, Gray RJ, Hernandez JL, Grant CS, Donohue JH. Breast cancer: presentation and intervention in women with gastrointestinal metastasis and carcinomatosis. Ann Surg Oncol. 2005;12(11):886-894. doipubmed
Critchley AC, Harvey J, Carr M, Iwuchukwu O. Synchronous gastric and colonic metastases of invasive lobular breast carcinoma: case report and review of the literature. Ann R Coll Surg Engl. 2011;93(5):e49-50. doipubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.