

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 11, Number 6, June 2020, pages 145-147
A Rare Case of Submucosal Fibroid Presented With Acute Abdomen: A Case Report
Julia Tana, b, Mohamed Siraja
aDepartment of Obstetrics and Gynaecology, KK Women’s and Children’s Hospital, 100 Bukit Timah Road, Singapore 229899, Singapore
bCorresponding Author: Julia Tan, Department of Obstetrics and Gynaecology, KK Women’s and Children’s Hospital, 100 Bukit Timah Road, Singapore 229899, Singapore
Manuscript submitted March 26, 2018, accepted April 3, 2018, published online May 28, 2020
Short title: Submucosal Fibroid Presented With Acute Abdomen
doi: https://doi.org/10.14740/jmc3049w
| Abstract | ▴Top |
Spontaneous bleeding from uterine leiomyoma is an unusual cause of hemoperitoneum. Fewer than 100 cases have been reported in the literature so far. We report a 30-year-old woman who needed surgical exploration for an acute abdomen. There was massive hemoperitoneum due to bleeding from a subserosal myoma. This case was important because physician should be aware of this rare complication in patient with uterine myoma to avoid any morbidity and mortality.
Keywords: Fibroid; Submucosal fibroid; Acute abdomen
| Introduction | ▴Top |
Uterine fibroids are common benign tumors in women. However, acute complications necessitating emergency surgical intervention are rare. We report a case of spontaneous rupture of feeding vessel of uterine fibroid needing emergency laparotomy.
| Case Report | ▴Top |
A 30-year-old lady, nulliparous, presented to the emergency department with acute onset of lower abdominal pain for 1 day. She has medical history of hypertension and asthma. Her menstrual cycle was normal and urine pregnancy test was negative. On examination, she had diffuse tenderness in the abdomen. A bedside abdominal sonogram was performed which revealed a large amount of free fluid. She was stable and went for a computed tomography (CT) of the abdomen and pelvis which showed hemoperitoneum with source of bleeding arising from a large uterine mass that has ruptured (Fig. 1). The hemoglobin level initially was 11.6 g/dL.
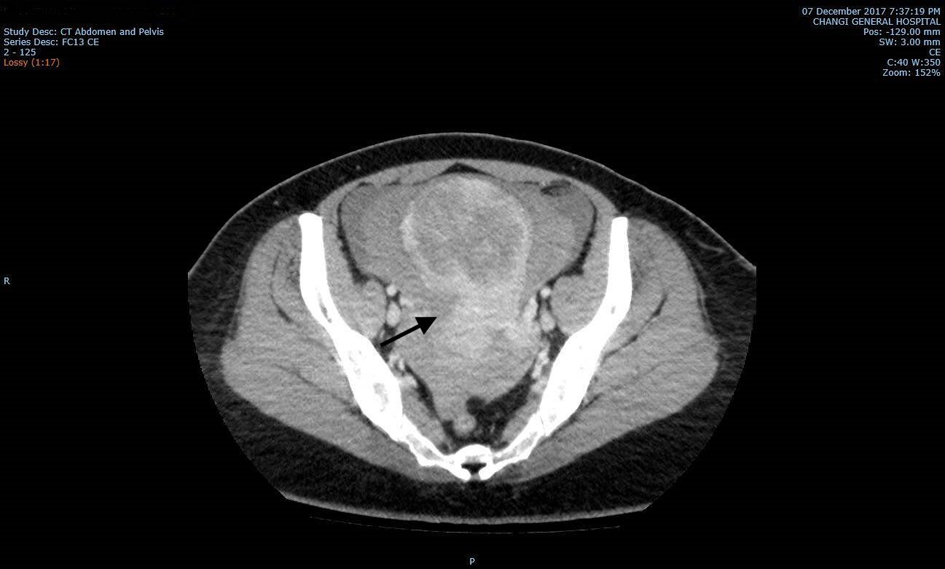 Click for large image | Figure 1. CT image showed hemoperitoneum with source of bleeding arising from a large uterine mass that has ruptured. CT: computed tomography. |
Patient went for emergency diagnostic laparoscopy. Upon entry by laparoscopy, a 9-cm pedunculated subserosal uterine leiomyoma was found, with a ruptured feeding vessel identified at the base of the fibroid. Decision was made to convert to open myomectomy in view of the active bleeding. The leiomyoma was excised and 1.3 L of blood and blood clots were evacuated from the peritoneal cavity. The postoperative course was uneventful. Her postoperative hemoglobin level was 7 g/dL. The patient was given 1 U of packed red blood cells and iron injection. Histopathologic review of the specimen revealed a 9-cm leiomyoma with areas of infarction, hemorrhage and vascular congestion (Figs. 2, 3).
 Click for large image | Figure 2. Active bleeding from the vein overlying a myoma. |
 Click for large image | Figure 3. Specimen of the excised myoma. |
| Discussion | ▴Top |
Uterine fibroids constitute the most common tumor in women of reproductive age. Most women with fibroids are asymptomatic. However, when clinically apparent, women usually experience heavy or prolonged menstrual bleeding or pelvic pressure. Acute complications secondary to fibroids are rare and seldom necessitate emergency surgical intervention. The complications include venous thromboembolism, acute pain secondary to degeneration or torsion of a pedunculated fibroid, acute urinary retention and subsequent renal failure [1]. It is rare for a uterine fibroid to spontaneously rupture [2].
Intraperitoneal hemorrhage from rupture fibroid is usually venous and secondary to an increase in abdominal pressure, which causes rupture of superficial veins [3]. Bleeding can also be arterial and usually associated with hypertension. Trauma causing avulsion of a fibroid, torsion of a pedunculated fibroid, and pregnancy causing venous congestion resulting in vessel rupture are other possible etiologies for intra-abdominal bleeding from a fibroid [4-6]. With regard to our case, we could not demonstrate any cause that could lead to rupture of the vessel.
Imaging modalities can aid in diagnosis of hemoperitoneum. The differential diagnosis between ascites and hemoperitoneum is sometimes not easy. Ultrasound is a helpful instrument to make a diagnosis of hemoperitoneum. CT could help the clinician to arrive at the correct diagnosis quickly. However, CT and ultrasound may not be able to delineate the origin of the bleeding [7]. Prompt emergency surgical intervention can be life-saving in situations such as the case described.
Conclusions
Rupture of uterine fibroid is rare, but it should be included in the differential diagnosis when encountering patient with known submucosa fibroid and acute abdomen pain. Exploratory laparotomy is both diagnostic and therapeutic in this life-threatening condition.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
Informed consent has been obtained from the individual included in this study.
Author Contributions
JT prepared first and subsequent drafts; MS contributed to the concept and review of all drafts; all authors discussed the findings and commented on the manuscript.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Okolo S. Incidence, aetiology and epidemiology of uterine fibroids. Best Pract Res Clin Obstet Gynaecol. 2008;22(4):571-588.
doi pubmed - Wallach EE, Vlahos NF. Uterine myomas: an overview of development, clinical features, and management. Obstet Gynecol. 2004;104(2):393-406.
doi pubmed - Buttery BW. Spontaneous haemoperitoneum from rupture of a uterine vein overlying a leiomyoma. Am J Obstet Gynecol. 1982:136:415.
doi - Takai H, Tani H, Matsushita H. Rupture of a degenerated uterine fibroid as a cause of acute abdomen: a case report. J Reprod Med. 2013;58(1-2):72-74.
- Danikas D, Theodorou SJ, Kotrotsios J, Sills C, Cordero PE. Hemoperitoneum from spontaneous bleeding of a uterine leiomyoma: a case report. Am Surg. 1999;65(12):1180-1182.
- Deopuria RH. Haemoperitoneum secondary to rupture of coronary veins on a fibroid uterus (Review). The Journal of Obstetrics and Gynecology of India. 1970;20:409-413.
- Kamat NV, Telkar HB, Ramani SK, Thakker AP. Ruptured degenerated uterine fibroid diagnosed by imaging. Obstet Gynecol. 2001;98(5 Pt 2):961-963.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.