

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://www.journalmc.org |
Case Report
Volume 12, Number 8, August 2021, pages 325-327

Surgical Removal of a Pacemaker Lead Entrapped by a Chiari Network: A Case Report
Takenori Sakaia, Yoshimi Satoa, Tatsuya Kawasakia, c, Hideki Takahashib
aDepartment of Cardiology, Matsushita Memorial Hospital, Moriguchi, Osaka, Japan
bTakahashi Clinic, Neyagawa, Osaka, Japan
cCorresponding Author: Tatsuya Kawasaki, Department of Cardiology, Matsushita Memorial Hospital, Sotojima 5-55, Moriguchi, Osaka 570-8540, Japan
Manuscript submitted May 1, 2021, accepted May 17, 2021, published online July 3, 2021
Short title: Pacemaker Lead Entrapped by Chiari Network
doi: https://doi.org/10.14740/jmc3708
| Abstract | ▴Top |
The Chiari network, one of the remnants of the right valve of the sinus venosus, is considered clinically insignificant in most cases but attention should be paid since this embryological remnant can be a potential risk for complications during procedures. We report a case of atrioventricular block in which a pacemaker lead was entrapped by a Chiari network. A 78-year-old woman underwent dual-chamber pacemaker implantation for symptomatic 2:1 atrioventricular block. A tined J-shaped atrial lead was placed at the right atrial appendage, which later became dislodged to a lower position and entrapped. After multiple unsuccessful attempts to withdraw the lead, surgical removal was performed. The lead was strictly entangled within the fibrous threads of the Chiari network that was not detected by transthoracic echocardiography before and during the implantation.
Keywords: Chiari network; Complication; Echocardiography; Lead; Pacemaker
| Introduction | ▴Top |
The Chiari network, one of the remnants of the right valve of the sinus venosus, is characteristic of fenestrated membranous or reticular structure in the valve of the inferior vena cava and coronary sinus [1, 2]. The Chiari network is considered clinically insignificant in most cases but attention should be paid to this embryological remnant since a Chiari network can be associated with cardiac events, such as thrombus and arrhythmia, as well as therapeutic complications [1]. We report a case of atrioventricular block in which a tined J-shaped atrial lead was entrapped by a Chiari network, although not recognized on echocardiography before and during the procedure, and was surgically removed.
| Case Report | ▴Top |
Investigations
A 78-year-old woman was admitted to Matsushita Memorial Hospital for the treatment of atrioventricular block. The patient was in a normal state of health until 2 weeks before presentation, when dyspnea on effort developed. A diagnosis of 2:1 atrioventricular block was made at another facility and she was referred to this hospital. Her previous medical history included hypertension and operation for a tumor of the parotid gland. Her medications were azilsartan at a dose of 20 mg daily and herbal medicine, Shakuyaku-Kanzo-To, at a dose of 2.5 g daily. The patient occasionally drank, did not smoke or use illicit drugs, and had no known allergies. There was no family history of cardiovascular disease.
Diagnosis
She was alert and did not seem sick, but looked lean with a height of 153.2 cm and weight of 41.2 kg (body mass index: 17.6 kg/m2). On examination, the blood pressure was 132/71 mm Hg, pulse was 49 beats per minute and regular, body temperature was 36.2 °C, and oxygen saturation was 98% while breathing ambient air. The jugular venous pressure was not high, but the third heart sound was audible at the apex with a grade 2 systolic ejection murmur. No pulmonary rales were heard and there was no edema in the legs.
Electrocardiography demonstrated bradycardia with a heart rate of 45 beats per minute, a normal axis, atrioventricular block with 2:1 conduction, and left ventricular high voltage. Chest radiography revealed cardiomegaly with a cardiothoracic ratio of 58% without pleural effusion or pulmonary congestion. The complete blood cell counts were normal, as were the levels of renal and liver function tests, electrolyte balance, and thyroid function test. The level of brain natriuretic peptide was 36.9 pg/mL (reference value ≤ 18.4). No remarkable findings were demonstrated on echocardiography; no Chiari network was detected.
Treatment
Dual-chamber pacemaker implantation was scheduled after obtaining informed consent from the patient. A 6.0-Fr guiding catheter was inserted via the left subclavian vein using the Seldinger technique, and was advanced close to the interventricular septum from the right ventricle. A 4.1-Fr ventricular lead (SelectSecure MRI SureScan 3830, Medtronic, Minneapolis, MN, USA) was screwed into the right ventricular side of the interventricular septum. A tined J-shaped 5.3-Fr atrial lead (CapSure Sense MRI SureScan 4574, Medtronic, Minneapolis, MN, USA) was placed at the right atrial appendage. During removal of the guiding catheter of the ventricular lead, the tined atrial lead became dislodged to a lower position and entrapped.
A removal procedure was performed by pulling the lead and using a gooseneck snare with the support of an 8.0-Fr catheter, without success. Given the contrast images via the 8.0-Fr catheter (Fig. 1), the dislodged atrial lead was likely to be entrapped by the tricuspid valve, but echocardiography was not informative regarding the entrapment site due to insufficient image quality. A Chiari network as well as Thebesian and Eustachian valves was also considered as a possible cause of the entrapment because echocardiography did not show an increase in tricuspid regurgitation by pulling the entrapped lead.
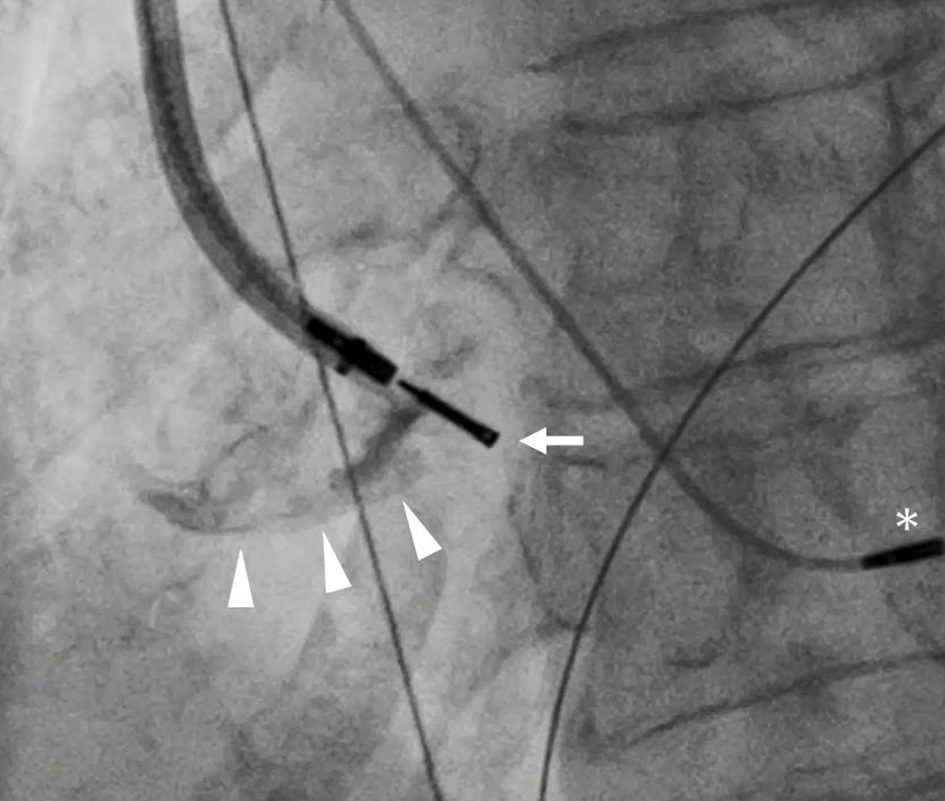 Click for large image | Figure 1. Contrast material via an 8.0-Fr guiding catheter proceeding close to the tip of the entrapped atrial lead (arrow) implies the borderline of the right atrium (arrowheads). There was no evidence of tricuspid regurgitation when the catheter and entrapped atrial lead were forcefully pulled. The asterisk shows a ventricular lead screwed into the interventricular septum. |
Following multiple unsuccessful attempts to withdraw the lead for 3 h, surgical removal was decided to be performed. The patient was transferred to another hospital and the atrial lead was surgically removed with a thoracotomy and right atriotomy. The lead was reported to be strictly entangled within the fibrous threads of the Chiari network and resection was required to remove the lead from the network. The patient underwent pacemaker implantation with epicardial electrodes. The clinical course was complicated by wound infection, which was treated with antibiotics and debridement. She was discharged to home and had been scheduled to visit Matsushita Memorial Hospital for a pacemaker check at regular intervals.
| Discussion | ▴Top |
We experienced a case of atrioventricular block requiring pacemaker implantation. Although a Chiari network was not detected on transthoracic echocardiography performed before and during the procedure, a tined J-shaped atrial lead was entrapped by a Chiari network and emergency surgery was needed to remove the lead.
This network was named after Hans Chiari who reported this condition in an autopsy series in 1897 [3], although initially described in the literature by von Rokitansky in 1875 [1]. The presence of a Chiari network, due to incomplete reabsorption of the right valve of the sinus venosus, is not uncommon regardless of age or gender, e.g., a 2% prevalence in 1,436 patients who underwent transesophageal echocardiography [4]. The presence of a Chiari network is likely to be associated with other heart diseases including a patent foramen ovale and atrial septal aneurysm, possibly leading to an increase in thrombotic events [4]. Loukas et al proposed the hypothesis that the Chiari network traps a small embolism and initiates the development of a larger thrombus [1].
It is also worth noting that attention should be paid to Chiari networks since the network might entrap medical devices such as pacemaker leads [5-7], catheters [8, 9], and even wires [10, 11], although the incidence of complications associated with Chiari networks remains unknown. On these occasions, surgical removal is generally selected after multiple unsuccessful attempts at removal, as in the current patient. However, less invasive methods may also be worth being considered before surgery is recommended. For example, it is reported that intracardiac echocardiography and a laser sheath were useful to remove a pacing lead entanglement within a Chiari network [6], although the availability may be limited. An entrapped lead can also be used for atrial sensing, instead of its extraction, if an intraatrial P wave potential can be recorded by the entrapped lead [7]. This was not applied in our case because the possibility that the lead might have been entrapped not in a Chiari network but in the tricuspid valve could not be denied.
Factors associated with lead entrapment in a Chiari network remain to be elucidated, but it is intuitive that a tined J-shaped lead, as used in the current patient, can become entrapped more easily than non-tined and/or non-J-shaped leads, although limited evidence is available. Given no echocardiographic evidence indicative of the presence of a Chiari network in the current patient, lead selection may be important to avoid unpredictable complications related to Chiari networks. This may be supported by the fact that passive atrial lead fixation (i.e., tined leads) was one of the independent predictors for complications within 2 months [12], although the usage of J-shaped active fixation atrial leads was associated with a higher incidence of pericardial irritation and/or effusion than J-shaped passive fixation atrial leads [13]. In a prospective, randomized, control study comparing the performance of J-shaped and straight atrial leads with an active (i.e., screw-in) fixation mechanism, both groups demonstrated favorable lead performance over a 5-year follow-up period [14].
In conclusion, our case highlights the importance of recognizing the Chiari network as a potential risk for complications during percutaneous transluminal procedures even in patients in which a Chiari network is not detected on transthoracic echocardiography beforehand.
Acknowledgments
The authors thank Dr. Tonai Kohei for his comments on the surgical findings.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
Not applicable because the manuscript has been sufficiently de-identified to protect the patient.
Author Contributions
TS, YS, and TK contributed to data analysis and study design; TS and TK wrote the paper; YS and HT reviewed the paper; all authors gave the final approval.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Loukas M, Sullivan A, Tubbs RS, Weinhaus AJ, Derderian T, Hanna M. Chiari's network: review of the literature. Surg Radiol Anat. 2010;32(10):895-901.
doi pubmed - Jansirani DD, Deep SS, Anandaraja S. Anatomical study of chiari network and the remnant of left venous valve in the interior of right atrium. Anat Res Int. 2015;2015:247680.
doi pubmed - Chiari H. Ueber Netzbildungen im rechten Vorhofe des Herzens, Beitr. z. path. Anat Uz allg Path. 1897;22:1-7.
- Schneider B, Hofmann T, Justen MH, Meinertz T. Chiari's network: normal anatomic variant or risk factor for arterial embolic events? J Am Coll Cardiol. 1995;26(1):203-210.
doi - Barakat K, Robinson NM, Dymond DS. Instantaneous lead entrapment: successful percutaneous removal using the cook workstation. Pacing Clin Electrophysiol. 1998;21(4 Pt 1):774-775.
doi pubmed - Aung H, Espinosa RE, Powell BD, McLeod CJ. Entrapment of a pacing lead within a chiari network: utility of intracardiac echo and a laser sheath. Pacing Clin Electrophysiol. 2016;39(6):620-622.
doi pubmed - Maruyama T, Kurogouchi F. Entrapment of a tined lead by the chiari network with preserved atrial sensing ability in a patient with atrioventricular block: a case report. J Cardiol. 2004;44(6):251-254.
- Chu S, Solheim E, Chen J, Hoff PI, Schuster P. Entrapment and retrieval of a diagnostic electrophysiological catheter in the Chiari network. J Arrhythm. 2018;34(6):647-649.
doi pubmed - Sakamoto A, Urushida T, Sakakibara T, Sano M, Suwa K, Saitoh T, Saotome M, et al. Accidental entrapment of electrical mapping catheter by Chiari's network in right atrium during catheter ablation procedure. Case Rep Cardiol. 2016;2016:1302473.
doi pubmed - Shimoike E, Ueda N, Maruyama T, Kaji Y, Niho Y. Entrapment of a guide wire by the Chiari network in a patient with ablated idiopathic ventricular tachycardia. J Interv Card Electrophysiol. 2001;5(2):219-222.
doi pubmed - Zhu W, Jin Z, Li Q. Entrapment of guide wire by Chiari's network during pacemaker implantation. Cardiol J. 2019;26(5):607.
doi pubmed - Udo EO, Zuithoff NP, van Hemel NM, de Cock CC, Hendriks T, Doevendans PA, Moons KG. Incidence and predictors of short- and long-term complications in pacemaker therapy: the FOLLOWPACE study. Heart Rhythm. 2012;9(5):728-735.
doi pubmed - Luria DM, Feinberg MS, Gurevitz OT, Bar-Lev DS, Granit C, Tanami N, Eldar M, et al. Randomized comparison of J-shaped atrial leads with and without active fixation mechanism. Pacing Clin Electrophysiol. 2007;30(3):412-417.
doi pubmed - Luria D, Bar-Lev D, Gurevitz O, Granit H, Rotstein Z, Eldar M, Glikson M. Long-term performance of screw-in atrial pacing leads: a randomized comparison of J-shaped and straight leads. Pacing Clin Electrophysiol. 2005;28(9):898-902.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.