

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 1, Number 2, October 2010, pages 68-70
Anomalous V-shape Palmaris Longus Tendon: Two Cases
Ali A. Alshahama, b, Paw Mulara, Kadhim Jawada
aDepartment of Surgery, International Medical School, Management and Science University, Malaysia
bCorresponding author: Department of Surgery, International Medical School, Management and Science University, Off Jalan Persiaran Olahraga, Seksyen 13, 40100 Shah Alam, Malaysia
Manuscript accepted for publication July 15, 2010
Short title: Palmaris Longus Tendon
doi: https://doi.org/10.4021/jmc114e
| Abstract | ▴Top |
We describe an incidental rare finding of V-shape tendon of Palmaris Longus (PL) in two cases. Examination of 253 subjects/506 hands for detection of PL Tendon by the standard clinical tests was undergone. The sample mean age was 21 years and M/F ratio was 1:3.The identification of V-shape bifid tendon was revealed only by Schaeffer’s test whiles both Thompson’s and Mishra’s tests failed to demonstrate the anomaly. These two cases with anomalous tendon did not provoke any symptom. The importance of this finding being a potential source of V-shape support that can be used as tendon transfer to extensor tendons, in restoration procedure of radial palsy, and as free transplant in reanimation of oral and lid angles in facial palsy or any where when a V-shape support is required. Therefore surgeon awareness of this anomalous tendon and pre-operative identification is warranted.
Keywords: Multiple anatomic variations; Palmaris longus; Flexor carpi ulnaris; Persistent median artery; Clinical significance
| Introduction | ▴Top |
The Palmaris Longus (PL) is the most variable muscle in the human arm and one of the most variable muscles in the human body [1, 2]. This variability has formed the base for many medical literatures. Although the PL muscle of little functional importance, it assumes great surgical importance since it is the first option in tendon graft procedures, for it is readily detected in vitro and easy surgical accessibility as well, which make harvesting its tendon much easier than its counterpart, the Plantaris muscle in the leg [3, 4]. The awareness of PL absence and the anomalous presentation is highly warranted. Reimann et al examined 1,600 extremities and found incidence rate of other anomalies apart from absence was 9% [5]. Furthermore concomitant anomalies in the soft tissue of the upper limb which share same embryonic origin (mesoderm) have been recorded as well [6-8]; these include nerves, arteries and other muscles. Therefore, knowledge of these anomalous structures, although rare, is important not only to anatomists but also to clinicians in their routine practice. The morphologic aspect of V-shape anomalous tendon and literatures review is presented with special emphasis on clinical significance of this anomalous finding.
| Case Report | ▴Top |
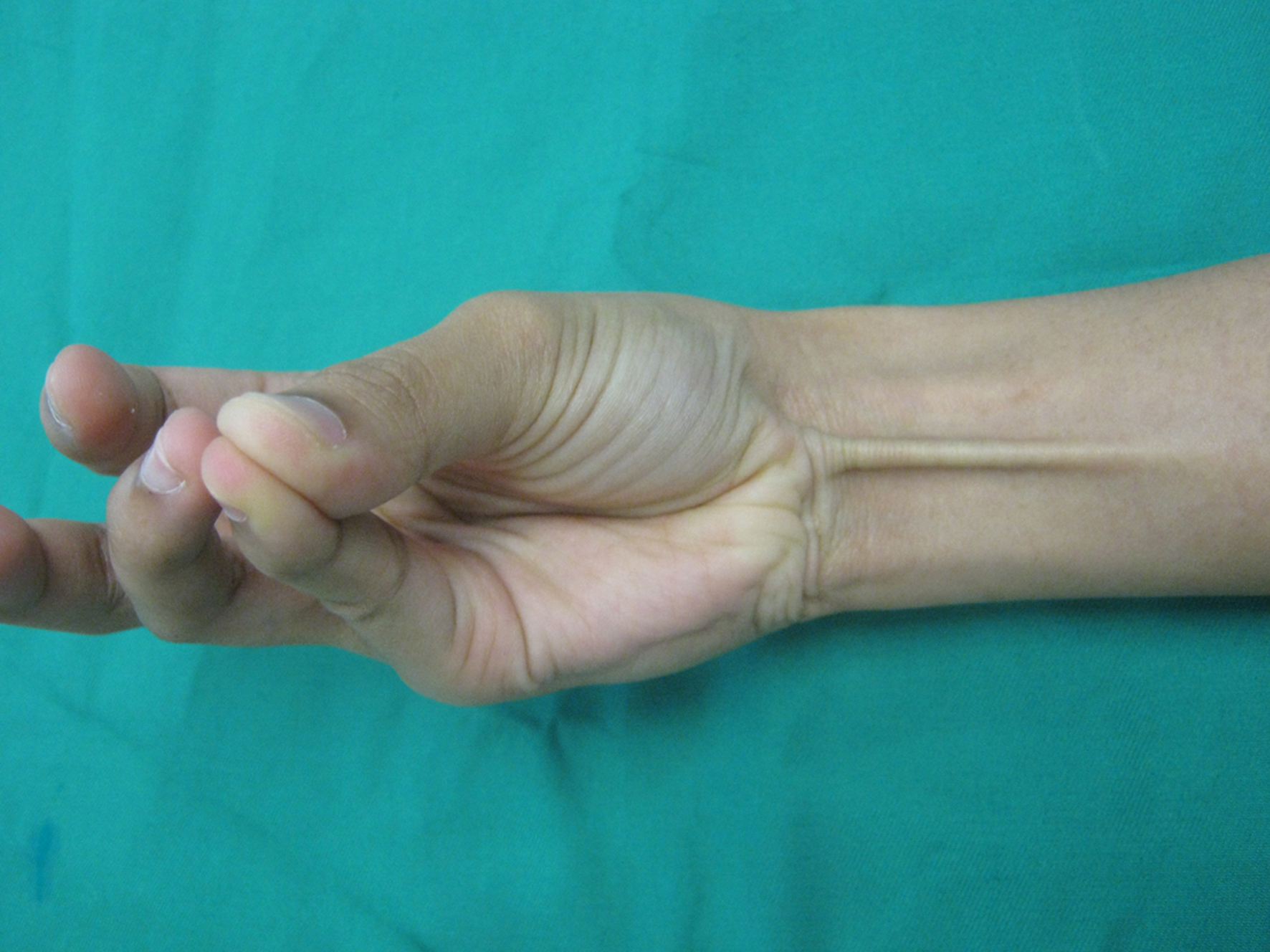
A prospective study to identify prevalence of absence of PL muscle among the medical school students of Faculty of Medicine, University Technology Mara were conducted, the examined sample of subjects: n = 253; hands: n = 506; the age ranged 19 - 22 years with the mean of 21 and the Male/Female ratio 1:3. Two asymptomatic cases were incidentally found during in vitro clinical examination by Schaeffer’s test (Fig. 1), while Thompson’s and Mishra’s test failed to demonstrate the anomalous tendon. The morphologic feature of the anomalous tendon was V-shape bifid distal part of PL tendon. Both slips run superficially crossing the wrist creases to be inserted into the palm onto palmer aponeurosis, the central tendoneus slip runs towards a groove created by the two eminences, in the mid-palm while the other lateral slip was radial directed towards the thenar eminence. This bifidity of the PL tendon was confirmed by wrist ultrasonography.
 Click for large image | Figure 1. Anomalous V-shaped PL identified in Schaeffer’s and not in Thompson’s or Mishra’s. |
| Discussion | ▴Top |
Palmaris Longus is often described as one of the most variable muscles in the human body and is classified as a phylogenetically retrogressive muscle, in other words, a short belly with a long tendon [9]. The PL absence is easy to detect in vitro by Schaeffer’s, Thompson’s and Mishra’s tests. Its absence ranged between 2.8-24% in different races [1, 2], but the reported incidence of other anomalies in the PL was still 9% (Table 1), including inverted PL [10, 11], three headed reversed [12], epifasial accessory [13], duplicate [14-16]. The muscle belly may be central, distal or digastrics or may be completely muscular [15]. According to Paraskevas et al, the duplication of palmaris longus vary between 0.8-3.1% [17].
 Click to view | Table 1. Types of Anomalies in Palmaris Longus |
The clinical significance of the anomalous PL was reported in numerous literatures. There are many reports of median and/or ulnar nerve compression due to the existence of a variant PL [18-20]. In clinical practice, the aberrant PL could also be incidentally found during clinical examination without provoking any clinical symptoms like our cases [18].
The PL tendon is often considered as an ideal donor tendon in hand surgery. It’s the first option in tendon grafts procedure of the long flexors, extensor tendons of the fingers, flexor pollicis longus tendon and extensor tendon defects as well. It can be used in tendon transfer procedure [13]. It is also utilized as a simple static support in the treatment of facial paralysis, and some surgeon utilize the tendon in digital pulley reconstruction [21], lip augmentation, and in various nerve palsies.
This unique V-shape arrangement of PL tendon makes it a potential source to provide V-shape splint in selected reconstructive procedures, oral and lid angle in facial palsy or any other reconstructive procedures where a V-shaped splint is required. Therefore, surgeon awareness of this anomaly, as well as pre-operative identification is warranted when such type of splint is indicated, and it can be easily distinguished from the normal PL tendon(Fig. 2).
 Click for large image | Figure 2. Single PL identified in Schaeffer’s test. |
In conclusion, the V-shape PL tendon represent potential donor splint in selected surgical procedures. Therefore surgeon awareness and pre-operative identification of this anomalous tendon is warranted.
| References | ▴Top |
- Thompson NW, Mockford BJ, Cran GW. Absence of the palmaris longus muscle: a population study. Ulster Med J 2001;70(1):22-24.
pubmed - Sebastin SJ, Lim AY. Clinical assessment of absence of the palmaris longus and its association with other anatomical anomalies— a Chinese population study. Ann Acad Med Singapore 2006;35(4):249-253.
pubmed - George R. Co-incidence of palmaris longus and plantaris muscles. Anat Rec 1953;116(4):521-523.
pubmed doi - Vanderhooft E. The frequency of and relationship between the palmaris longus and plantaris tendons. Am J Orthop (Belle Mead NJ) 1996;25(1):38-41.
pubmed - Reimann AF,Daseler EH,Anson BJ,Beaton LE.The Palmaris longus muscle and tendon:astudy of 1600 extrimities. anat Rec 1944;89:495-505.
- Coskun N, Sarikcioglu L, Donmez BO, Sindel M. Arterial, neural and muscular variations in the upper limb. Folia Morphol (Warsz) 2005;64(4):347-352.
pubmed - Rodriguez-Niedenfuhr M, Sanudo JR, Vazquez T, Nearn L, Logan B, Parkin I. Median artery revisited. J Anat 1999;195 (Pt 1)(57-63.
pubmed - Chalmers J. Unusual causes of peripheral nerve compression. Hand 1978;10(2):168-175.
pubmed - Zeybek A, Gurunluoglu R, Cavdar S, Bayramicli M. A clinical reminder: a palmaris longus muscle variation. Ann Plast Surg 1998;41(2):224-225.
pubmed doi - Oommen A, Rajarajeshwari T. Palmaris Longus – Upside Down! J Anat. Soc. India 2002;51(2):232-233.
- Ruiz Santiago F, Moyano Calvente S, Ruiz Sanchez F. [Keys for the diagnosis of inverted palmaris longus muscle by ultrasound]. Radiologia 2006;48(6):391-393.
pubmed doi - Natsis K, Levva S, Totlis T, Anastasopoulos N, Paraskevas G. Three-headed reversed palmaris longus muscle and its clinical significance. Ann Anat 2007;189(1):97-101.
pubmed - Tiengo C, Macchi V, Stecco C, Bassetto F, De Caro R. Epifascial accessory palmaris longus muscle. Clin Anat 2006;19(6):554-557.
pubmed doi - Kawashima T, Kikushima S, Yokota E, Ohkubo F, Yamana Y, Sato F, Sasaki H. A case of an accessory palmaris longus muscle and a duplicate palmaris longus muscle with special reference to their nerve supply—morphologic significance of a common innervation trunk. Okajimas Folia Anat Jpn 2002;79(2-3):75-81.
pubmed doi - Hojo T. A case of the duplicate palmaris longus muscle. Kaibogaku Zasshi 1976;51(6):422-425.
pubmed - Saadeh FA, Bergman RA. Doubled palmaris longus muscle (with accessorius ad flexorem minimi digiti). Anat Anz 1986;161(5):393-395.
pubmed - Paraskevas G, Tzaveas A, Natsis K, Kitsoulis P, Spyridakis I. Failure of palmaris longus muscle duplication and its clinical application. Folia Morphol (Warsz) 2008;67(2):150-153.
pubmed - Georgiev GP, Jelev L, Surchev L. Reversed palmaris longus muscle simulating soft-tissue mass as a possible cause of median nerve compression. J Orthop Trauma (Bulgaria) 2008; 45: 92-4.
- Turner MS, Caird DM. Anomalous muscles and ulnar nerve compression at the wrist. Hand 1977;9(2):140-142.
pubmed - Acikel C, Ulkur E, Karagoz H, Celikoz B. Effort-related compression of median and ulnar nerves as a result of reversed three-headed and hypertrophied palmaris longus muscle with extension of Guyon's canal. Scand J Plast Reconstr Surg Hand Surg 2007;41(1):45-47.
pubmed doi - Kaufmann RA, Pacek CA. Pulley reconstruction using palmaris longus autograft after repeat trigger release. J Hand Surg Br 2006;31(3):285-287.
pubmed doi
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.