

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 3, Number 3, June 2012, pages 172-173
Double Pylorus: An Uncommon Endoscopic Finding
Onur Keskina, Irfan Soykana, b
aAnkara University Faculty of Medicine, Ibni Sina Hospital, Division of Gastroenterology Ankara, Turkey
bCorresponding author: Irfan Soykan, Ankara University Faculty of Medicine, Ibni Sina Hospital, Division of Gastroenterology, 06100 Sihhiye, Ankara, Turkey
Manuscript accepted for publication January 27, 2012
Short title: Double Pylorus
doi: https://doi.org/10.4021/jmc552e
| Abstract | ▴Top |
Fistulas that occur between the stomach and duodenum give the appearance of a “double pylorus. This is a rare endoscopic finding and it can be either congenital or acquired as in most of the cases which occurs as a complication of peptic ulcer disease and less frequently as a complication of gastric malignancy. In this report we present the endoscopic findings of two patients with double pylorus one patient occuring as a result of peptic ulcer disease and the other one is resulting from gastric malignancy.
Keywords: Double pylorus; Peptic ulcer disease; Gastric carcinoma
| Introduction | ▴Top |
Double pylorus is a fistulous communication between the gastric antrum and the bulbus of the duodenum. It is generally silent clinically and can be presented with dyspeptic symptoms such as epigastric pain, nausea and bloating. However, double pylorus is mostly found incidentally during endoscopic or radiolgic investigation [1].
| Case Report | ▴Top |
Case 1
A 56-year-old man underwent esophagogastroduodenoscopy due to epigastric pain and abdominal bloating. The esophagogastroduodenoscopy noted two channels in the gastric antrum, in which one of them is true pylorus and the other one is fistulae tract. The scope was able to enter the duodenum through the pylorus but not from the fistulae tract. There was no evidence of active peptic ulcer disease, however an ulcer scar was observed between pylorus and adjacent channel (Fig. 1). Gastric biopsies revealed evidence of Helicobacter pylori infection and treated by pantoprazole, amoxycilline and clarythromycine and followed by proton pump inhibitors.
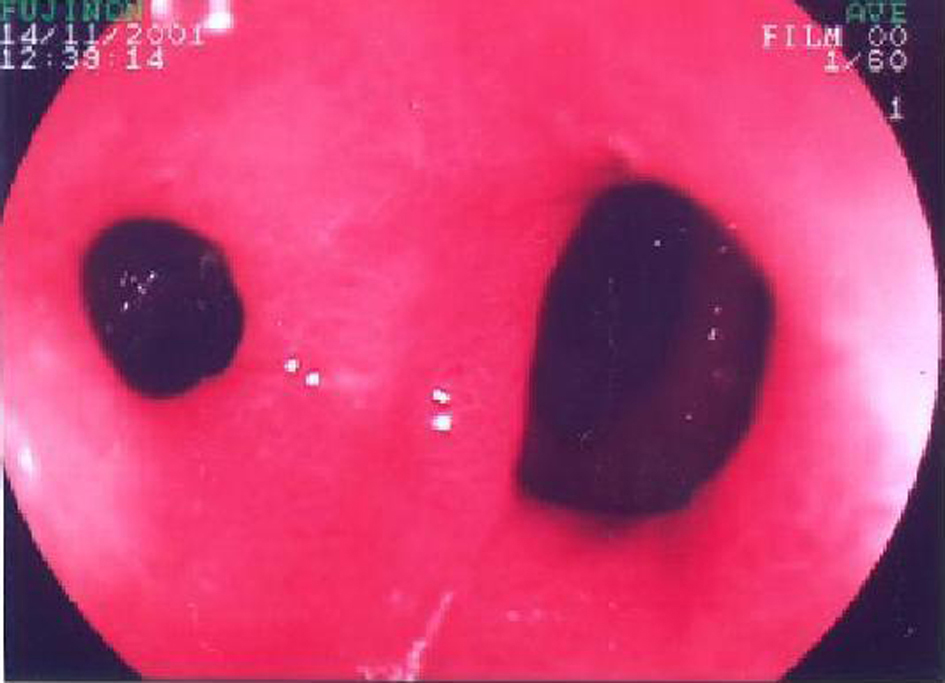 Click for large image | Figure 1. Endoscopic view illustrating pylorus and a second opening just close to the pylorus with minimal scarring between two channels. |
Case 2
A 75-year-old man with a history of long-term epigastric pain and recent onset of nausea, vomiting and weight loss underwent gastroscopic examination. The gastroscopy revealed deformed bulbus and pyloric ring and a fistulae-like irregular opening just above the pylorus on the minor curvatura of the gatric antrum with surrounding inflammation (Fig. 2). The scope entered the duodenum with difficulty but we could not be able to pass through fistula. Helicobacter pylori infection was found to be positive in gastric biopsies, however the patient did not respond well to medical therapy and needed surgical treatment revealing gastric carcinoma fistulised to bulbus.
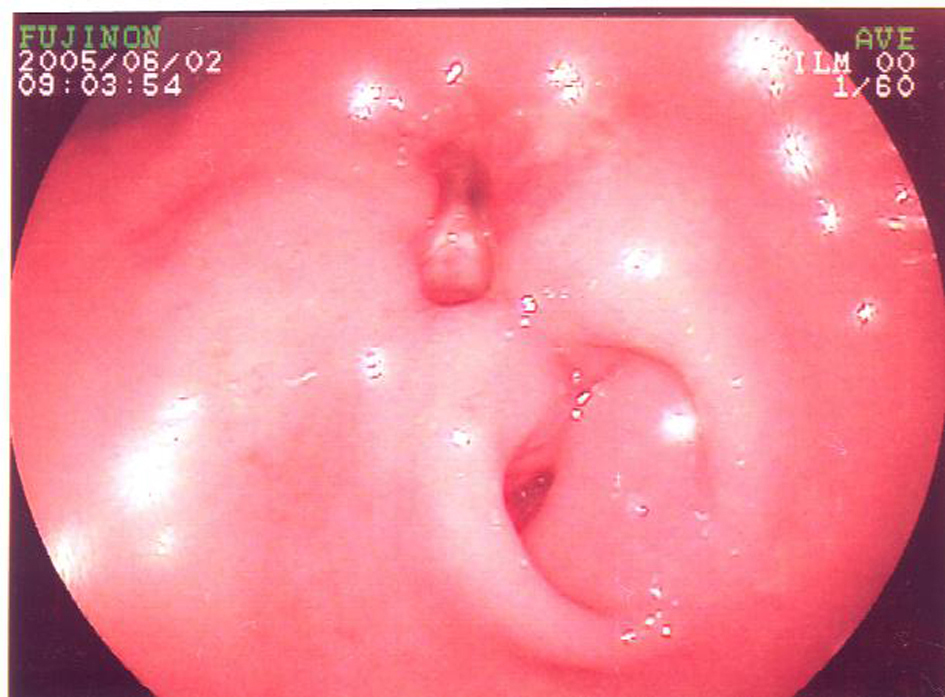 Click for large image | Figure 2. Endoscopic image showing deformed bulbus and pyloric ring and a fistulae-like opening just above the pylorus on the minor curvatura of the gatric antrum with surrounding inflammation. |
| Discussion | ▴Top |
Double pylorus is a fistulous connection between the gastric antrum and the bulbus of the duodenum and it is generally associated with peptic ulcer disease [1]. In addition to peptic ulcer disease, it has been reported as a congenital disorder and may develop as a consequence of gastric carcinoma. Double pylorus is also associated with systemic diseases such as diabetes mellitus, hypertension, chronic renal failure, chronic obstructive lung diseases and ulcerogenic medications [2]. Pyloric dublications which appear as cysts and diverticula may mimick double pylorus, however they are not true channels and are extremely rare conditions. The reported prevalence of double pylorus is estimated between 0.02% and 0.4% and majority of the fistulas are located on the minor curvatura of the antrum [2, 3]. In the clinical setting, double pylorus can present itself with epigastric pain, dyspeptic symptoms and upper gastrointestinal bleeding or can be found incidentally [4]. Treatment of this condition is mostly conservative, however patients who exhibit a more refractory progress may have underlying gastric carcinoma necessitating surgical therapy.
Grant Support
None.
Conflict of Interest
None.
| References | ▴Top |
- Lee TH, Park SH. Double pylorus secondary to recurrent ulcer: serial endoscopy follow-up. Endoscopy. 2008;40 Suppl 2:E226.
pubmed - Hu TH, Tsai TL, Hsu CC, Lu SN, Hsiao M, Changchien CS. Clinical characteristics of double pylorus. Gastrointest Endosc. 2001;54(4):464-470.
pubmed doi - Hegedus V, Poulsen PE, Reichardt J. The natural history of the double pylorus. Radiology. 1978;126(1):29-34.
pubmed - Akazawa Y, Mizuta Y, Osabe M, Nakamura T, Morikawa S, Isomoto H, Takeshima F, et al. A case of double pylorus caused by recurrent gastric ulcers: a long-term endoscopic observation. Dig Dis Sci. 2005;50(11):2125-2128.
pubmed doi
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.