

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 4, Number 3, March 2013, pages 161-162
Laparoscopic Management With Detorsion Suture of an Ovarian Torsion During Early Pregnancy
Murat Apia, Hakan Aytana, Raziye Narinb, c, Hakan Nazikb, Mehmet Ali Narinb, Cevdet Adıguzelb
aDepartment of Obstetrics and Gynecology, Numune Education and Research Hospital, Adana, Turkey
bDepartment of Obstetrics and Gynecology, Numune Education and Research Hospital, Adana, Turkey
cCorresponding author: Raziye Narin, Adana Numune Education and Research Hospital, Adana, Turkey
Manuscript accepted for publication November 20, 2012
Short title: Laparoscopic Management
doi: https://doi.org/10.4021/jmc1026e
| Abstract | ▴Top |
The aim of the study is to present a case of maternal adnexal torsion at the 9th gestational weeks, and its laparoscopic management with prophylactic detorsion suture. A 22-year-old, gravida 3, spontaneous abortion 2, pregnant woman at her 9th weeks of gestation, presented to the emergency department with acute onset of excruciating pain in the left and right-abdominal quadrant. Laboratory results were normal. In the right adnexa, a large, 10 cm х 6 cm edematous ovary was seen. Laparoscopy was performed with a standart technics. A congested 10 cm right ovary was found to be twisted around its adnexal pedicle 2.5 rotations. After untwisting the ovarian pedicle, the ovary returned to its normal color and showed no signs of hemorrhage or necrosis. The patient recovered without problems and discharged on the first postoperative day. The remainder of her pregnancy was unremarkable.
Keywords: Torsion; Early pregnancy; Laparoscopic suture; Detorsion
| Introduction | ▴Top |
Ovarian torsion is the total or partial rotation of the adnexa around its vascular axis. Venous or lymphatic blockade could result in potentially massive enlargement of the ovary caused by continued arterial inflow to the ovary without venous outflow. Eventually, if undiagnosed and untreated, arterial stasis can lead to hemorrhagic infarction and necrosis of the ovarian stroma. The risk of ovarian torsion rises by 5 fold during pregnancy. Incidence is 5 per 10,000 pregnancies [1]. Its most common cause in pregnancy is a corpus luteum cyst, which usually regresses spontaneously by the second trimester [2]. Ovarian torsion, therefore, occurs most frequently in the first trimester, occasionally in the second, and rarely in the third [3]. Recurrence rate of torsion was 19.5% in pregnant women [4]. Ovarian fixation is an alternative method to cystectomy for preventing recurrence [5]. The aim of the study is to present a case of maternal adnexal torsion at the 9th gestational weeks, and its laparoscopic management with prophylactic detorsion suture.
| Case Report | ▴Top |
A 22-year-old, gravida 3, spontaneous abortion 2, pregnant woman at her 9th weeks of gestation, presented to the emergency department with acute onset of excruciating pain in the left and right-abdominal quadrant. She reported no vaginal bleeding or discharge, nausea, vomiting, fever, diarrhea, or constipation. Her general and gynecologic history was noncontributory.
Physical examination showed she was diaphoretic. Her vital signs were unremarkable for a blood pressure of 120/85 mmHg and a pulse of 88 beats/min. Abdominal examination revealed a palpable right lower quadrant mass below the level of the umbilicus, with voluntary guarding but no rebound or peritoneal signs. Pelvic examination revealed a 10-week sized soft uterus, with a closed cervix, and a tender 10-cm right adnexal mass.
Laboratory results were normal. Transvaginal sonography performed at the examination room visualized a normal fetus in utero with a gestational age of 9 weeks. In the right adnexa, a large, 10 cm х 6 cm edematous ovary was seen. The left ovary appeared normal, and some free fluid was seen in the cul-de-sac. With color flow doppler small cystic masses periferally located at the right ovary and some vascular flow were identified at the perifery of the ovary. With a presumptive diagnosis of ovarian torsion, the patient was brought to the operating room, where general anesthesia and endotracheal intubation were carried out. Laparoscopy was performed with a standart 10 mm main trochar at the umblical level, and two satellite 5 mm trochars at the inguinal regions. On entry into the abdominal cavity with a main trochar at the umblicus, a congested 10-cm right ovary was found to be twisted around its adnexal pedicle 2.5 rotations (Fig. 1). After untwisting the ovarian pedicle, the ovary returned to its normal color and showed no signs of hemorrhage or necrosis. Since the patient was pregnant the luteo-placental hormonal mileu was probably still acting, so the ovary was not incised. Oophoropexy was performed with a no 0 polyglactin 910 suture material with blunt needle to fix the ovary to the ovarian fossa with peritoneal serosal intracorporeal suturing technique. The patient recovered without problems and was discharged on the first postoperative day. The remainder of her pregnancy was unremarkable.
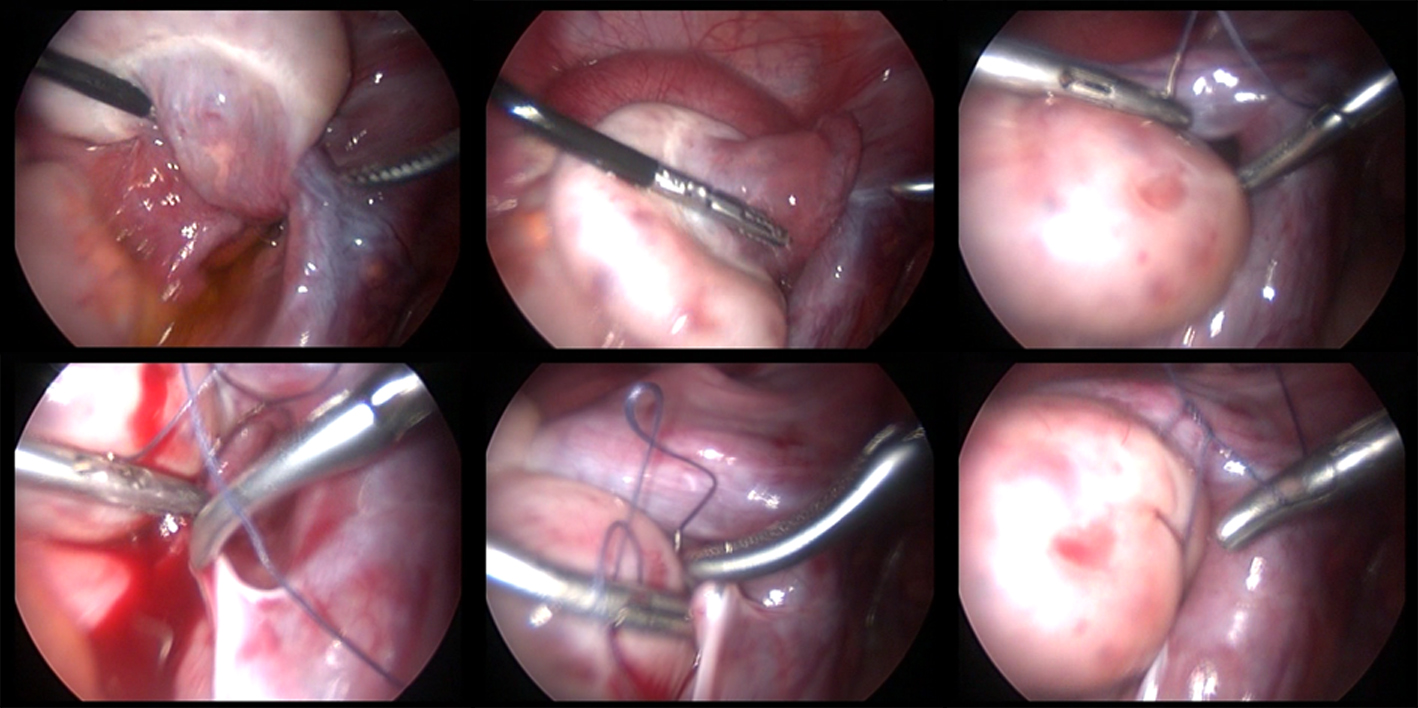 Click for large image | Figure 1. Right adnexal torsion (upper left) and detorsion (upper middle), ovarian fixation sutures to the peritoneum of the fossa ovarica. |
| Discussion | ▴Top |
Expedient surgery is a requisite treatment for ovarian torsion. The decision to proceed to surgery during pregnancy is somewhat complex, since the well-being of both mother and fetus must be taken into account. The risk of any surgery to the pregnancy will depend on the gestational age. In the first trimester, when ovarian torsion most often occurs in pregnancy, the risk of fetal loss is the smallest with modern anesthetic techniques. For years, the treatment of choice for ovarian torsion was salpingooophorectomy. Conservative treatment appears to be warranted to preserve fertility, even for adnexa that initially appear nonviable and purple or black in color. A major consideration is whether the surgery can be performed by laparoscopy or by laparotomy. In the nonpregnant patient and during the first trimester of pregnancy, ovarian torsion can usually be approached laparoscopically.
Conclusion
Diagnosis of ovarian torsion can usually be made on the basis of the characteristic clinical presentation in conjunction with ultrasound evidence of a unilaterally enlarged adnexal mass. Treatment options are limited to surgery, either by laparoscopy or laparotomy, the former becomes more difficult in pregnancy but should be the treatment of choice if experienced surgeon and equipment is available. Theoretically cystectomy in early pregnancy may detoriate the corpus luteum function, so ovarian fixation may be more preferable.
Competing Interests
The authors declare that they have no competing interests.
| References | ▴Top |
- Kemmann E, Ghazi DM, Corsan GH. Adnexal torsion in menotropin-induced pregnancies. Obstet Gynecol. 1990;76(3 Pt 1):403-406.
pubmed - Duic Z, Kukura V, Ciglar S, Podobnik M, Podgajski M. Adnexal masses in pregnancy: a review of eight cases undergoing surgical management. Eur J Gynaecol Oncol. 2002;23(2):133-134.
pubmed - Hibbard LT. Adnexal torsion. Am J Obstet Gynecol. 1985;152(4):456-461.
pubmed - Hasson J, Tsafrir Z, Azem F, Bar-On S, Almog B, Mashiach R, Seidman D, et al. Comparison of adnexal torsion between pregnant and nonpregnant women. Am J Obstet Gynecol. 2010;202(6):536 e531-536.
- Weitzman VN, DiLuigi AJ, Maier DB, Nulsen JC. Prevention of recurrent adnexal torsion. Fertil Steril. 2008;90(5):2018 e2011-2013.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.