

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 9, Number 5, May 2018, pages 131-134
A Case of Cecal Cancer With Heterotopic Ossification
Ayaka Omoria, b, Hiroki Hashidaa, Satoshi Kaiharaa
aDepartment of Surgery, Kobe City Medical Center General Hospital, 2-1-1 Minatojima-Minamimachi, Chuo-ku, Kobe 650-0047, Japan
bCorresponding Author: Ayaka Omori, Department of Surgery, Kobe City Medical Center General Hospital, 2-1-1 Minatojima-Minamimachi, Chuo-ku, Kobe 650-0047, Japan
Manuscript submitted February 12, 2018, accepted February 26, 2018
Short title: Cecal Cancer With Ossification
doi: https://doi.org/10.14740/jmc3020w
| Abstract | ▴Top |
Heterotopic bone formation in the colon is rare, and its mechanism is still unclear. A 45-year-old man with severe anemia was referred to our hospital and was diagnosed as with cecal cancer on exploratory colonoscopy. On right hemicolectomy with lymphadenectomy, the cut surface of the resected specimen showed a type 2 tumor with a white solid lesion in the cecum. The histopathological study revealed a moderately differentiated adenocarcinoma with ossification. Herein we report and discuss this rare case.
Keywords: Colon cancer; Heterotopic bone formation; Ossification
| Introduction | ▴Top |
Heterotopic bone formation in malignant neoplasms is common in renal, liver, breast, and skin carcinomas; however, it is rare in the colon. In 1923, there was a first report on a colon cancer with ossification. In 1939, Dukes was the first investigator in the English literature to describe rectal cancer with ossification. The etiology and mechanism of heterotopic bone formation in the colon are still unclear. Therefore, we present a case of cecal cancer with ossification.
| Case Report | ▴Top |
A healthy 45-year-old man was referred to our hospital for severe anemia (hemoglobin level, 4.8 g/dL). A colonoscopy revealed an irregular protruding tumor in the cecum (Fig. 1), which was infiltrating the Bauhin valve (Fig. 2). Irrigoscopy showed the typical apple-core sign; the patient was diagnosed as having cecal cancer.
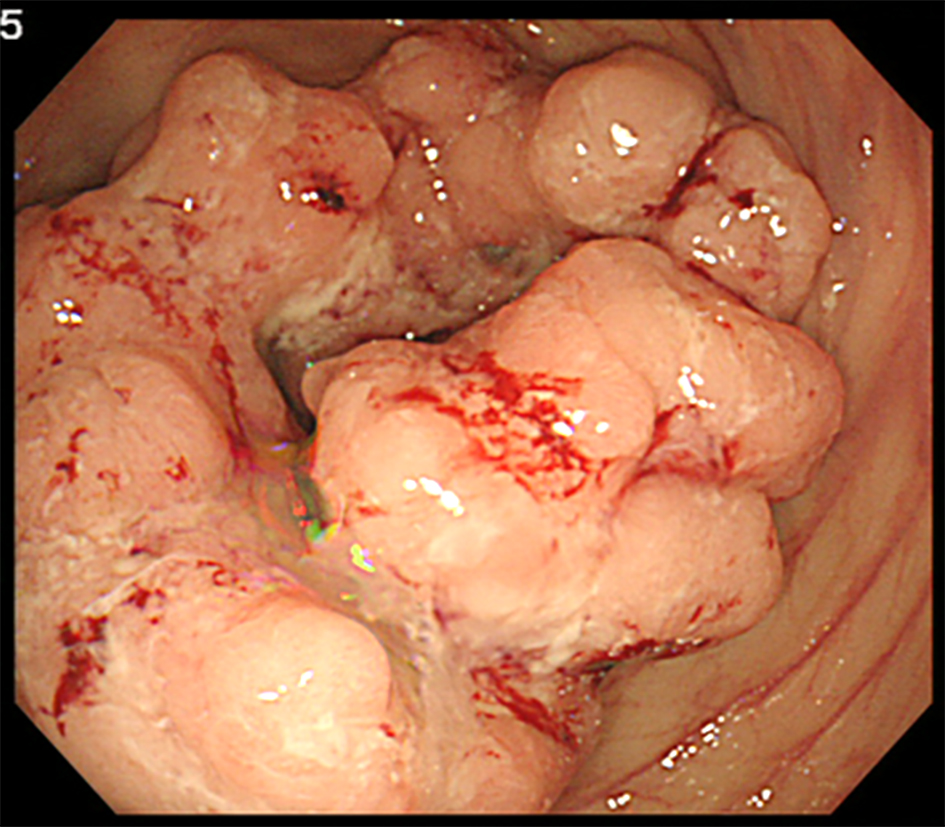 Click for large image | Figure 1. Colonoscopy revealing a cecal cancer with bleeding. |
 Click for large image | Figure 2. Irrigoscopy showing the typical apple-core sign at the cecum. |
The computed tomography scan showed an irregular cecal wall thickening without any signs of calcification or ossification. We observed several lymph node metastases around the cecum and the ileocolic arteries (Fig. 3); therefore, we performed a right hemicolectomy with a regional lymphadenectomy.
 Click for large image | Figure 3. Computed tomography scan showing an irregular cecal wall thickening without any sign of calcification or ossification. |
Pathological findings
The resected right hemicolon specimen contained a 70 × 65 mm mass with a white, solid region (Fig. 4). Cross-sections cut from the fixed tissue revealed a moderately differentiated adenocarcinoma with mucus collection. The tumor extended into the subserosal tissue, with absence of necrotic tissue. The white solid lesion comprised an ossification tissue with normal osteoblasts completely surrounded by the benign fibrous tissue. No histological evidence of venous or lymphatic invasion was observed. A total of 27 lymph nodes were recovered from the mesentery; no lymph node metastasis was observed (Fig. 5).
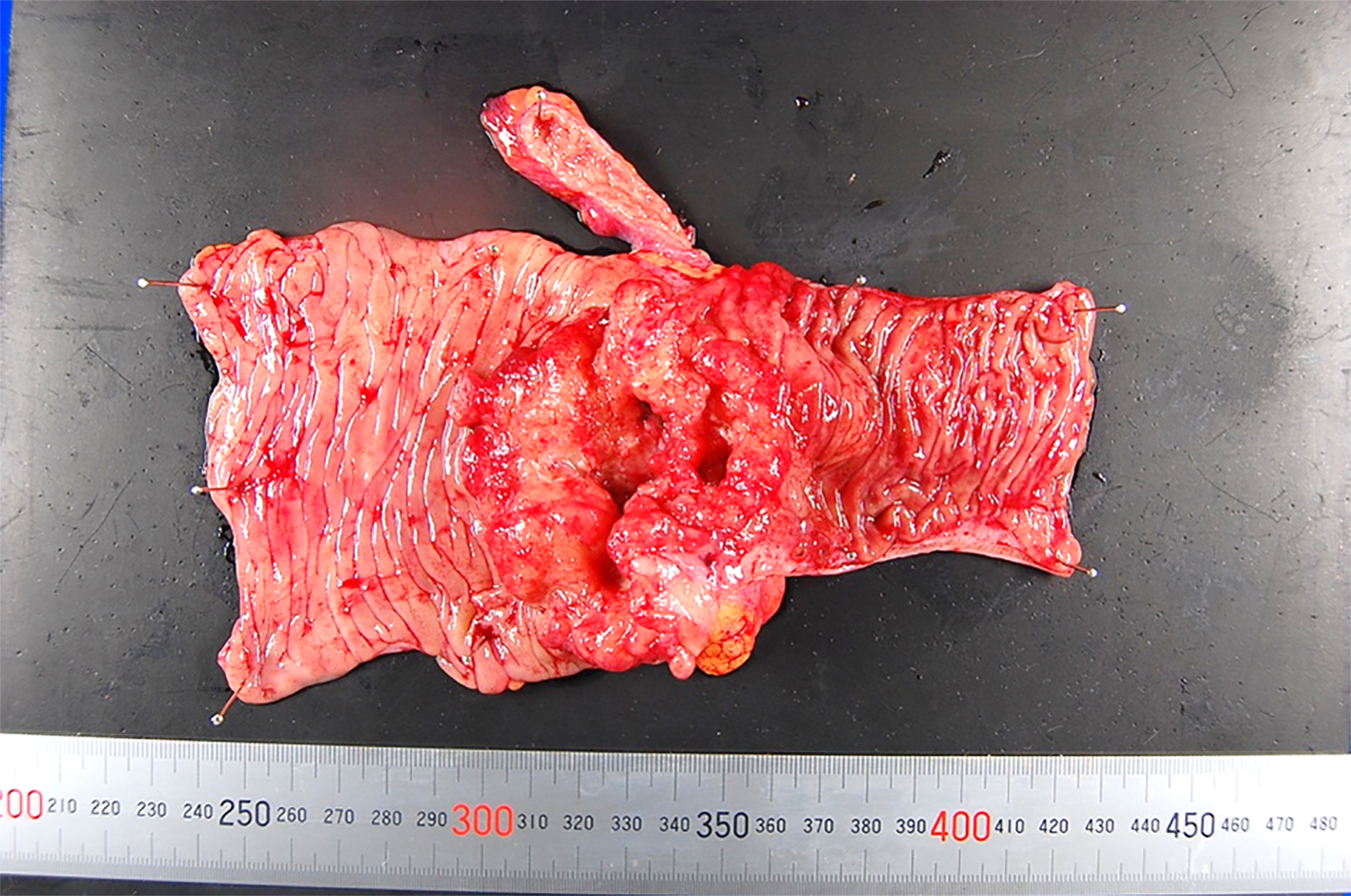 Click for large image | Figure 4. The resected specimen. |
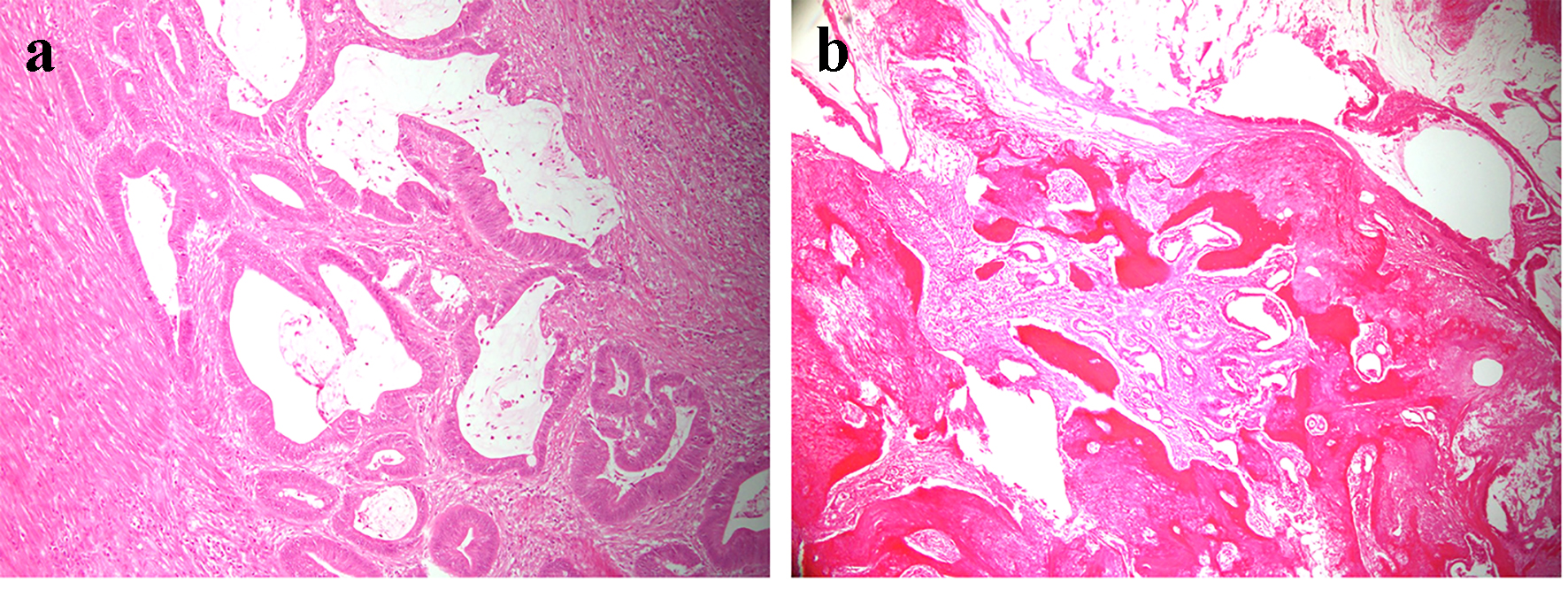 Click for large image | Figure 5. (a) A section of the main tumor comprising moderately differentiated adenocarcinoma tissue. (b) A section of the white solid lesion showing heterotopic bone formation without dysplasia. |
| Discussion | ▴Top |
Bone formation in the colon is a rare phenomenon. Colon cancer with ossification has been reported as a slowly progressive, moderately to highly differentiated tumor that is not invasive to vessels or lymph nodes. Mucosal and necrotic tissues often coexist [1-4].
Heterotopic bone formation has been observed within the tumor stroma associated with necrosis and within pools of mucus [3, 5-9]. However, most colon cancers with necrotic tissue are not associated with ossification, and not all colon cancers with ossification present with an associated necrotic tissue (similar to the tumor in our case). The association between tissue necrosis and bone formation is unclear; however, it is clear that the presence of necrosis is not a prerequisite for bone formation.
Two hypotheses have been proposed to explain the pathogenesis of heterotopic bone formation: osteoblastic metaplasia of cancer cells and pluripotent mesenchymal cells, both under the influence of factors generated by the cancer cells [5]. Electron microscopic studies in two cases of lung cancers have reported a lack of intermediate stages between tumor cells and osteoblasts [10]. Werner et al have demonstrated the transition from osteoblasts to fully differentiated osteocytes in gastric cancer of rats [11]. These reports suggest the osteoblastic metaplasia of normal mesenchymal cells. In our case, the ossification tissue with osteoblasts was completely surrounded by the benign fibrous tissue, suggesting that the osteoblasts were derived from the pluripotent mesenchymal cells and not the cancer cells.
There is no difference between colon cancer with and without ossification with respect to the course, management, and prognosis [5, 6]. Apart from colon cancer, osseous metaplasia has also been reported in association with benign polyps of the colon, carcinoids of the stomach, and mucoceles of the appendix [5, 8, 12].
Osseous metaplasia in colon cancer should not be confused with carcinosarcoma because although the latter is extremely rare, it has a much worse prognosis due to its more invasive nature and high recurrence rate [13]. Colon cancer with ossification can be differentiated from carcinosarcoma because the osseous metaplasia in colon cancer is always associated with benign bone formation, similar to this case [7].
As they have totally different prognoses, colon cancer with ossification needs to be differentiated from other benign lesions and carcinosarcomas. Only few colon cancer cases with ossification have been reported in the literature, and the pathophysiology is not well known. Further studies are needed to find the etiological, epidemiological, and pathophysiological factors associated with osseous metaplasia in colon cancer.
Conflict of Interest
The authors declare no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Grant Support
The authors received no financial support for the research, authorship, and/or publication of this article.
| References | ▴Top |
- Ansari MQ, Sachs IL, Max E, Alpert LC. Heterotopic bone formation in rectal carcinoma. Case report and literature review. Dig Dis Sci. 1992;37(10):1624-1629.
doi pubmed - Imai N, Iwai A, Hatakeyama S, Matsuzaki K, Kitagawa Y, Kato S, Hokari R, et al. Expression of bone morphogenetic proteins in colon carcinoma with heterotopic ossification. Pathol Int. 2001;51(8):643-648.
doi pubmed - Shevach MR. Calcification and ossification in a mucinous adenocarcinoma of the colon; report of a case. Am J Dig Dis. 1962;7:356-359.
doi pubmed - Stabler J. Case report: ossifying metastases from carcinoma of the large bowel demonstrated by bone scintigraphy. Clin Radiol. 1995;50(10):730-731.
doi - Kypson AP, Morphew E, Jones R, Gottfried MR, Seigler HF. Heterotopic ossification in rectal cancer: Rare finding with a novel proposed mechanism. J Surg Oncol. 2003;82(2):132-136; disccussion 137.
- Haque S, Eisen RN, West AB. Heterotopic bone formation in the gastrointestinal tract. Arch Pathol Lab Med. 1996;120(7):666-670.
pubmed - Lauwers GY, Wahl SJ, Richard GK. Osseous metaplasia in colonic adenocarcinoma. Am J Gastroenterol. 1991;86(3):382.
pubmed - Al-Maghrabi H, Jamison BM, Veinot JP. Calcified colonic mass. Arch Pathol Lab Med. 2005;129(10):1347-1348.
pubmed - Alper M, Akyurek N, Patiroglu TE, Yuksel O, Belenli O. Heterotopic bone formation in two cases of colon carcinoma. Scand J Gastroenterol. 2000;35(5):556-558.
doi pubmed - Byard RW, Thomas MJ. Osseous metaplasia within tumours. A review of 11 cases. Ann Pathol. 1988;8(1):64-66.
pubmed - Werner B, Dahm K, Breucker H. Ossification in cancer of the stomach: an experimental study. Z Krebsforsch Klin Onkol Cancer Res Clin Oncol. 1976;86(2):147-154.
doi pubmed - Sperling MH, Friedman CJ. Osseous metaplasia in a benign colon polyp. Gastrointest Endosc. 1981;27(3):198-199.
doi - Weidner N, Zekan P. Carcinosarcoma of the colon. Report of a unique case with light and immunohistochemical studies. Cancer. 1986;58(5):1126-1130.
doi
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.