

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website https://www.journalmc.org |
Case Report
Volume 12, Number 7, July 2021, pages 288-290
Vaginal Myomectomy and Total Vaginal Hysterectomy on Large Prolapsed Cervical Myoma: A Case Report
Frank M.M. Wageya, Rudy Lengkonga, Freddy W. Wageya, Hermie M.M. Tendeana, John J.E. Wantaniaa, Erna Suparmana, Bismarck J. Laihada, Suzanna P. Mongana, Linda M. Mamengkoa, Juneke J. Kaenga, M.M. Joice Sondakha, Yosep Sutandara, b, Maria Gladys Theresaa
aDepartment of Obstetrics and Gynecology, Faculty of Medicine Universitas Sam Ratulangi, Prof. Dr. R. D. Kandou General Hospital Manado, Manado, Indonesia
bCorresponding Author: Yosep Sutandar, Department of Obstetrics and Gynecology, Faculty of Medicine Universitas Sam Ratulangi, Prof. Dr. R. D. Kandou General Hospital Manado, Manado, Indonesia
Manuscript submitted April 5, 2021, accepted April 19, 2021, published online May 13, 2021
Short title: Vaginal Myomectomy on Prolapsed Cervical Myoma
doi: https://doi.org/10.14740/jmc3698
| Abstract | ▴Top |
Cervical myomas are benign tumors originating from cervical muscle tissue with a very rare incidence of only about 8% of all myomas. The surgical approach depends on the position of cervical myoma. This case report discusses a 44-year-old woman who complained of a lump discharge from her birth canal 6 months ago, and currently discharging from her vagina. We performed vaginal myomectomy, and the cervical myoma measuring 8 × 8 × 6 cm with solid consistency was removed. We continued with total vaginal hysterectomy. Post-operative recovery was progressing well. The histopathology report was consistent with leiomyoma. Large prolapsed cervical myoma can be disturbing and discomforting for many patients. It is relatively rare and can be successfully removed vaginally with minimal morbidity.
Keywords: Vaginal myomectomy; Total vaginal hysterectomy; Prolapsed; Cervical; Myoma
| Introduction | ▴Top |
Myomas are benign smooth muscle tumors that are most often found in women of reproductive age, given that their growth is influenced by the hormones estrogen and progesterone [1, 2]. The incidence of myomas in the world is 20-35%, while in Indonesia it is 2.4-11.7% [3]. Data in Prof. Dr. R. D. Kandou General Hospital Manado from 2013 to 2014 showed that myomas were the second largest gynecological tumor [4]. There are several types of myoma, one of which is cervical myoma. Cervical myoma is relatively rare, only about 8% of all myomas [5].
Myoma growth is influenced by several factors, such as early age of menarche, late menopause, black race, and family history of myoma, less parity, a diet high in red meat and low in vegetables and fruit, consumption of caffeine and alcohol, no exercise, the presence of radiation and infection or injury to the uterus [2]. Hormonal contraception, exposure to cigarette, stress levels, obesity, diabetes mellitus, and hypertension still have an inconsistent relationship with the incidence of myoma [2]. Usually these benign tumors do not cause symptoms, but in some cases can cause abnormal uterine bleeding, urinary retention, constipation, coitus problems, pain, and infertility [6, 7].
| Case Report | ▴Top |
A woman, 44 years old with para 3, abortion 0, came to the Prof. Dr. R.D. Kandou General Hospital with chief complaint of the discharge of a lump from the birth canal. The patient had felt a lump in her pubic area in the past 6 months, but only now did the lump come out of the birth canal. Complaints such as pain in the lump, the presence of vaginal discharge or bleeding out of the birth canal were denied. The patient also had no complaints about urinating and defecating. The patient complained of a feeling of fullness in the pubic area. Menarche was at 15 years of age with regular menstrual cycles every 28 - 30 days and a duration of 3 to 5 days. The patient had her last menstrual period in 2006. The patient has routinely used 3-month injection contraception since 2006 until now. The patient denied that she had menstrual irregularities or with profuse bleeding. At the time of examination, the patient appeared calm, with a blood pressure of 130/80 mm Hg, a pulse rate of 80 beats per minute, a respiratory rate of 20 times per minute, and a body temperature of 36.9 °C. The patient did not appear icteric or anemic. On examination of the abdomen, no abnormalities were found. On pelvic examination, a pink mass emerged from the vagina. The mass was 8 × 8 × 6 cm in size with a solid consistency (Fig. 1). An ultrasound examination showed that there was an adenomyosis appearance. We did biopsy of the cervical mass and the result was leiomyoma. After clinicopathological conference in our department, we decided to perform vaginal myomectomy, continued with total vaginal hysterectomy. The procedure was performed by an urogynecologist. A vaginal myomectomy was performed under general anesthesia. Intraoperatively, a leiomyoma that came out of the vagina with a hypertrophied cervix was found (Fig. 2). The leiomyoma was removed completely after it was clamped at the base and twisted. The base of the myoma was ligated with polyglycolic acid (PGA) No. 1 tapper. We continued with total vaginal hysterectomy. Estimated bleeding is about 200 mL. Post-operative recovery was good, and the patient was discharged on day 3. The patient came to control 3 days after going home with a good condition.
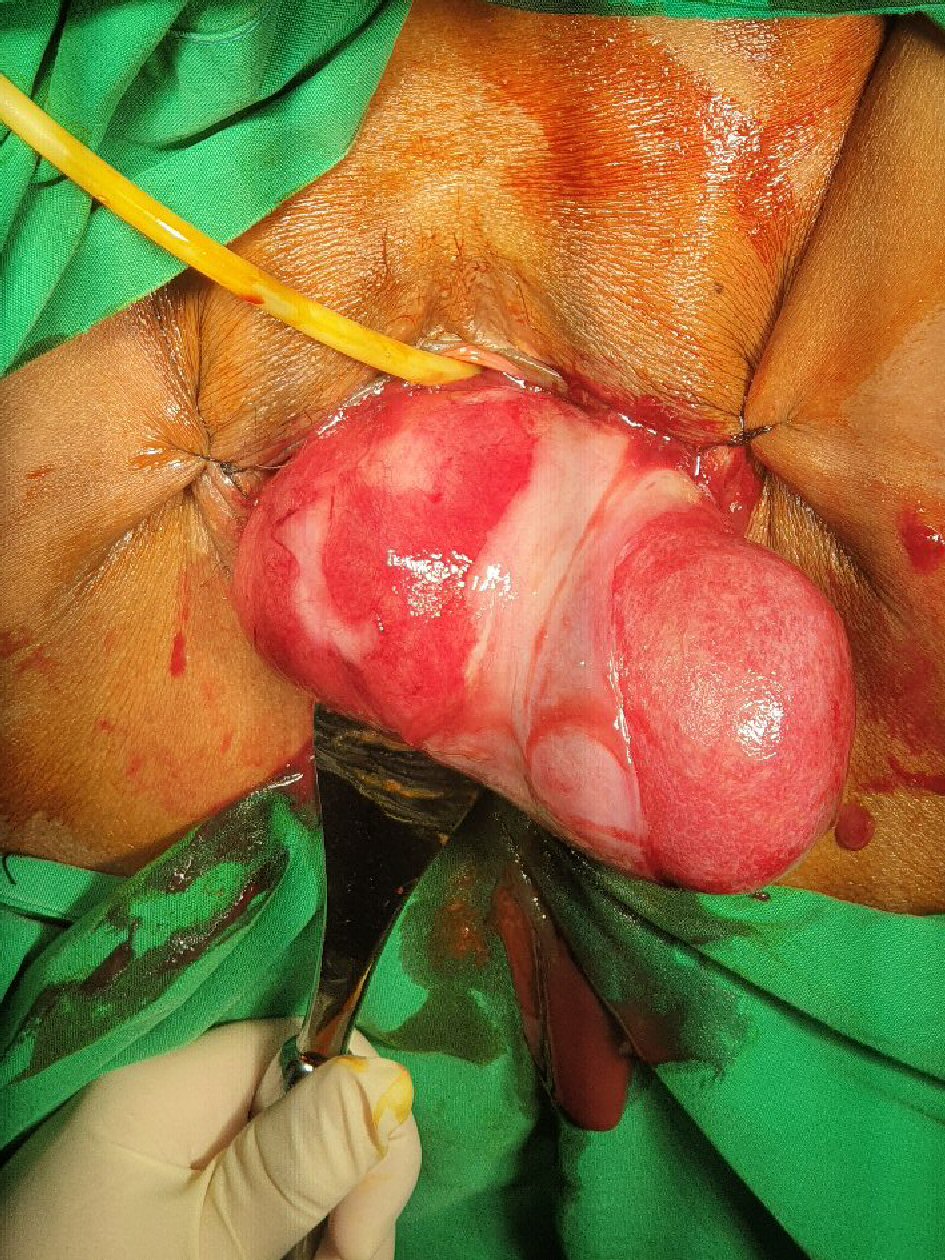 Click for large image | Figure 1. Cervical myoma before myomectomy. This large cervical mass prolapsed from the vaginal canal. |
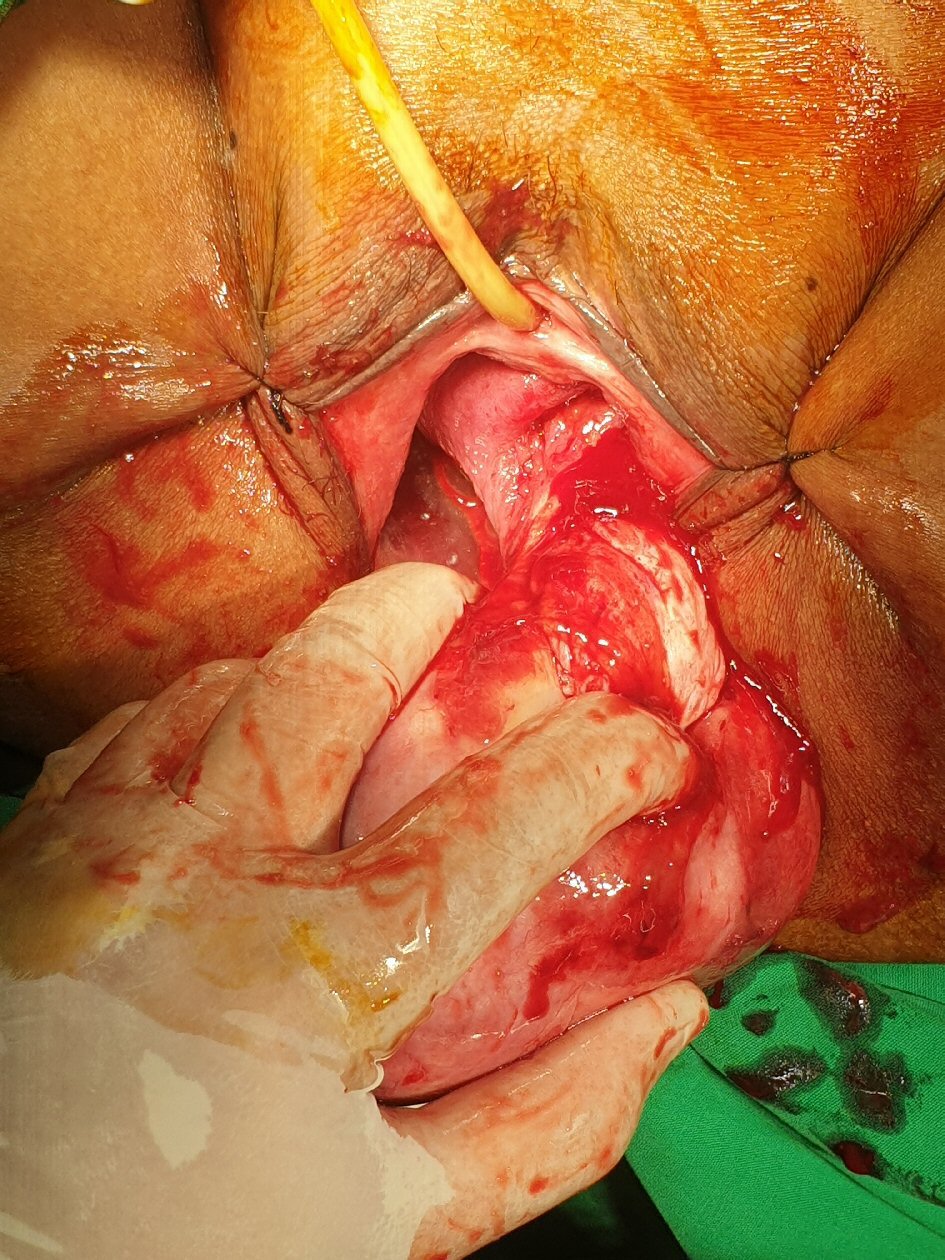 Click for large image | Figure 2. During the operation, the urogynecologist inspected thoroughly to identify the cervical canal. The myoma was located in the posterior aspect of the cervix. |
The histopathologic reports were as follow. From macroscopic appearance, the mass was well-circumscribed white-grey tissue with a glistening surface. It measured 8 × 8 × 6 cm and weighed ± 529 g (Fig. 3). From microscopic appearance it was consistent with leiomyoma with necrotic debris, focal edema, and focal infarction with signs of infection with neutrophil infiltrates. The final diagnosis was cervical leiomyoma.
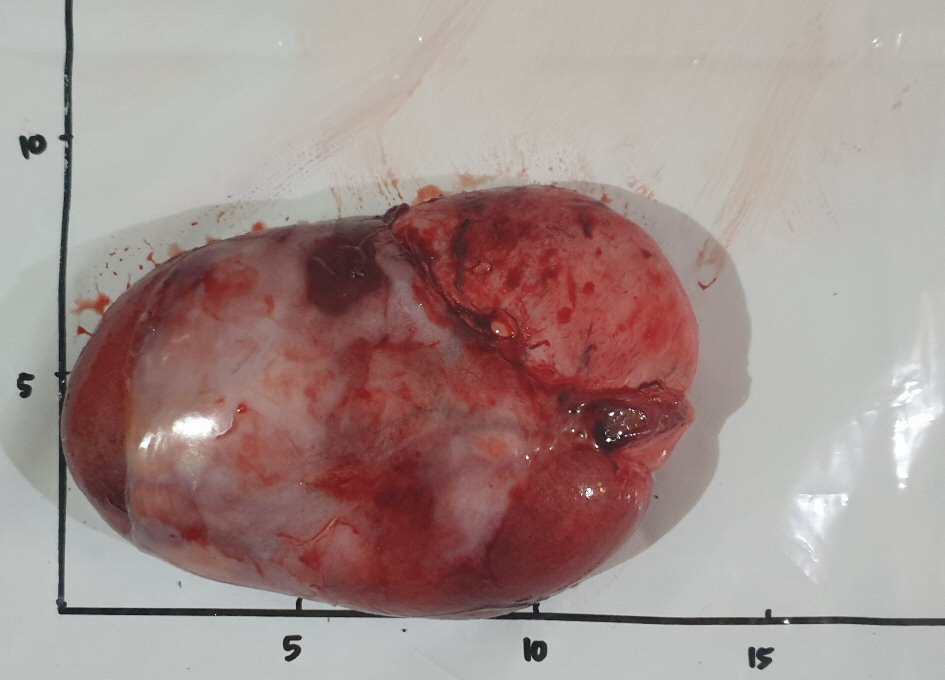 Click for large image | Figure 3. Macroscopic appearance of the cervical myoma right after the myomectomy. |
| Discussion | ▴Top |
Cervical myomas originate from cervical muscle tissue. Diagnosis of fibroid tumors must be through histopathological examination. Cervical myomas are usually solitary in nature in contrast to uterine myomas. It is not uncommon for cervical myomas to have a mass that comes out of the birth canal. This is because the myoma can prolapse out of the cervix [8]. Sometimes ulcers can form in prolapsed myomas due to inadequate blood circulation through the stalk [7].
Surgery performed for cervical fibroids can be vaginal or abdominal [9]. Vaginal myomectomy is the treatment of choice in cases of prolapsed myoma [10]. The type of surgery performed on a prolapsed myoma depends on several factors. Vaginal myomectomy is usually performed on young patients who still want to maintain their reproductive function. In patients who are older or have more than one myoma, hysterectomy is preferable [11]. The procedure for vaginal myomectomy is usually shorter and more practical, and in most patients no further management is required. The post-operative hospitalization period is also shorter than that of abdominal surgery [10].
Conclusions
Large prolapsed cervical myoma can be disturbing and discomforting for many patients. It is relatively rare and can be successfully removed vaginally with minimal morbidity. In this case, the surgery could improve the quality of life of the patient.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
There is no conflict of interest.
Informed Consent
Informed consent was obtained.
Author Contributions
Frank M. Wagey: writing of original draft; Rudy Lengkong: operator for the procedure; Freddy W. Wagey: investigation and diagnosis, writing of review and editing; Hermie M. M. Tendean: supervision; John J. E. Wantania: supervision; Erna Suparman: supervision; Bismarck J. Laihad: supervision; Suzanna P. Mongan: supervision; Linda M. Mamengko: supervision; Juneke J. Kaeng: supervision; Joice Sondakh: supervision; Yosep Sutandar: writing of original draft; Maria Gladys Theresa: writing of original draft.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Stewart EA, Cookson CL, Gandolfo RA, Schulze-Rath R. Epidemiology of uterine fibroids: a systematic review. BJOG. 2017;124(10):1501-1512.
doi pubmed - Sparic R, Mirkovic L, Malvasi A, Tinelli A. Epidemiology of uterine myomas: a review. Int J Fertil Steril. 2016;9(4):424-435.
- Ali B. Endokrinologi Ginekologi. 3rd ed. Jakarta: Media Aesculapius FKUI; 2008.
- Pasinggi S, Wagey F, Rarung M. Prevalensi Mioma Uteri Berdasarkan Umur di RSUP Prof. Dr. R. D. Kandou Manado. Jurnal e-Clinic. 2015;3.
doi - Tiltman AJ. Leiomyomas of the uterine cervix: a study of frequency. Int J Gynecol Pathol. 1998;17(3):231-234.
doi pubmed - Benassi L, Rossi T, Kaihura CT, Ricci L, Bedocchi L, Galanti B, Vadora E. Abdominal or vaginal hysterectomy for enlarged uteri: a randomized clinical trial. Am J Obstet Gynecol. 2002;187(6):1561-1565.
doi pubmed - Taingson MC, Adze JA, Bature SB, Amina DM, Caleb M, Amina A. Vaginal myomectomy of a large prolapsed cervical leiomyoma. Archives of International Surgery. 2016;6:3.
doi - Sengupta S, Reddy K, Pillai M. Prolapsed cervical fibroid in pregnancy: a challenging obstetric dilemma. J Obstet Gynaecol. 2006;26(8):823-824.
doi pubmed - Keriakos R, Maher M. Management of Cervical Fibroid during the Reproductive Period. Case Rep Obstet Gynecol. 2013;2013:984030.
doi pubmed - Ben-Baruch G, Schiff E, Menashe Y, Menczer J. Immediate and late outcome of vaginal myomectomy for prolapsed pedunculated submucous myoma. Obstet Gynecol. 1988;72(6):858-861.
doi pubmed - Dicker D, Feldberg D, Dekel A, Yeshaya A, Samuel N, Goldman JA. The management of prolapsed submucous fibroids. Aust N Z J Obstet Gynaecol. 1986;26(4):308-311.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.