

| Journal of Medical Cases, ISSN 1923-4155 print, 1923-4163 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Med Cases and Elmer Press Inc |
| Journal website http://www.journalmc.org |
Case Report
Volume 4, Number 2, February 2013, pages 89-91
A Scutum Presenting as a White Mass Behind an Intact Tympanic Membrane
Jeong Hwan Choia, b
aDepartment of Otolaryngology Head and Neck surgery, Sanggye Paik Hospital, College of Medicine, Inje University, Seoul, Korea
bCorresponding address: Department of Otorhinolaryngology, Inje University Sanggye Paik Hospital, 761-1 Sanggye-7-dong Nowon-gu, Seoul, 139-707, Republic of Korea (South)
Manuscript accepted for publication October 25, 2012
Short title: Scutum Presenting as White Mass
doi: https://doi.org/10.4021/jmc938w
| Abstract | ▴Top |
The lateral wall of the middle ear is formed largely by the tympanic membrane and to a lesser extent by scutum. A white mass behind an intact tympanic membrane is usually associated with congenital cholesteatoma, middle ear tympanosclerosis, middle ear adenoma and an osteoma of the ossicular chain. The scutum eggshell appearance caused by hyperpneumatization should not be mistaken for other pathologic conditions.
Keywords: Scutum
| Introduction | ▴Top |
The lateral wall of the middle ear is formed largely by the tympanic membrane and to a lesser extent by the bony outer attic wall extending from the squamous portion of the temporal bone called the scutum. A white mass behind an intact tympanic membrane is usually associated with congenital cholesteatoma, middle ear tympanosclerosis, middle ear adenoma and an osteoma of the ossicular chain [1]. There also has been a variable scutum anatomy. The eggshell appearance of scutum caused by hyperpneumatization should not be mistaken for other pathologic conditions.
| Case Report | ▴Top |
A 42-year-old female was admitted to our clinic with a several-week history of otalgia, itching and ear fullness, tinnitus and hearing loss in the both ear. There were no other complaints in the otorhinolaryngologic field and no recent history of trauma, otitis media or previous middle ear surgery. Otoscopy revealed diffuse ear canal edema and erythema. The tympanic membrane was not fully evaluated. After instillation of the steroid otic solution for a week, otoscopic examination revealed a white bulged mass like lesion at the postersuperior quadrants of the intact tympanic membrane (Fig. 1). Audiologic examinations including pure tone audiogram and tympanometry did not reveal any significant findings. Further imaging analysis was performed to clarify the lesion. Temporal bone computed tomographic scan (TBCT) demonstrated elongated scutum presenting as eggshell appearance (Fig. 2) and both mastoid processes were well pneumatized. This report was approved by the Inje University Sanggye Paik Hospital Institutional Review Board (SPIRB 12-021).
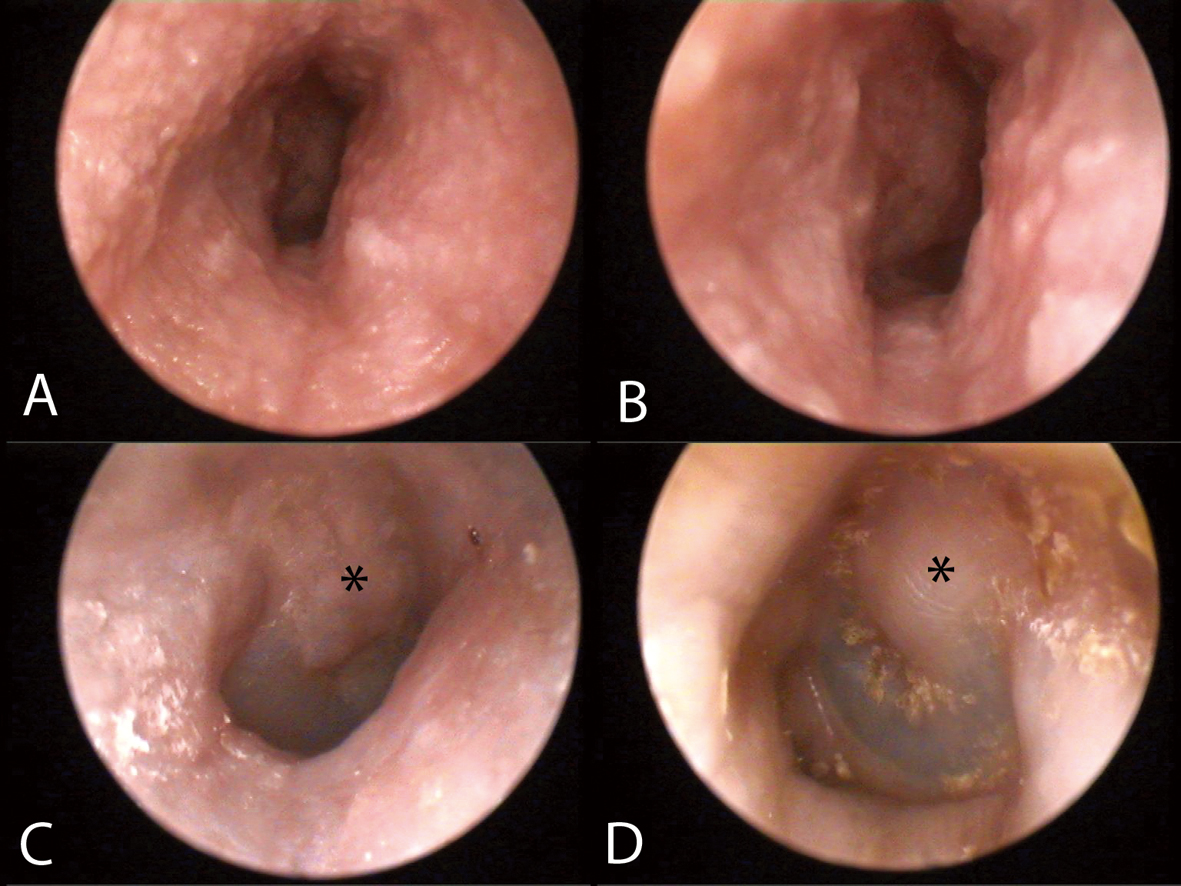 Click for large image | Figure 1. Otoscopic finding. Otoscopy revealed diffuse ear canal edema and erythema. A, B, the tympanic membrane was not fully evaluated. C, D, after instillation of the steroid otic solution for a week, otoscopic examination revealed a white bulged mass like lesion (*) at the postersuperior quadrants of the intact tympanic membrane. |
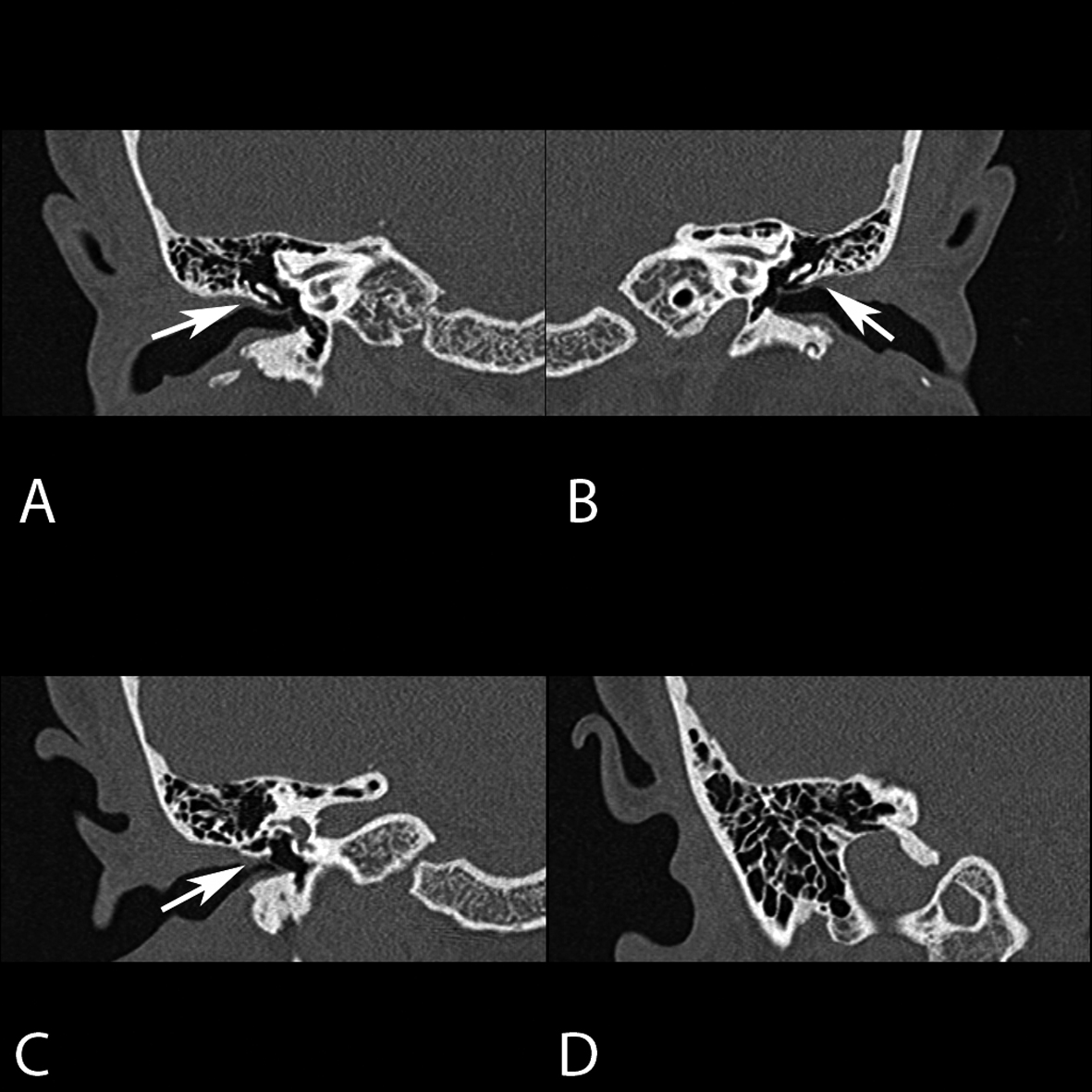 Click for large image | Figure 2. The computed tomographic coronal section of the temporal bone, bone window settings. A, B, C, the scan demonstrated elongated scutum (arrow) presenting as eggshell appearance. D, both mastoid processes are well pneumatized. |
| Discussion | ▴Top |
A white mass behind an intact tympanic membrane is usually associated with congenital or acquired cholesteatoma, middle ear tympanosclerosis, middle ear adenoma, or neuroma of the middle ear nerves. This appearance is also mimicked by a cartilage graft, an osteoma of the ossicular chain, and a foreign body [1]. These conditions should be evaluated because of neighboring organs which are important for hearing, balancing, and facial expression. Therefore, radiologic evaluation is inevitable. In this case the TBCT findings showed that the lesiona were not the part of skin or tympanic membrane itself but scutum.
The eggshell appearance of the scutum probably was due to hyperpneumatization. The normal process of the pneumatization of the temporal bone starts in the last weeks before birth with reduction of the embryonic mesenchyme in the antrum and progresses through infancy, childhood and puberty, when the last part of the petrous apex is pneumatized. Large pneumatization of the temporal squama, extending behind the sigmoid sinus, is considered to be a normal variant [2].
Extensive hyperpneumatization of the temporal and occipital bone usually has been reported in association with pneumatocele, which represents a spontaneous collection of gas, sually air, beneath the pericranium or within the skull. According to the study of Madeline [3], the occipitomastoidal synchondrosis remains partially opened into the teenage years or early adulthood, while the other synchondroses of the occipital bone close earlier. The lambdoid suture connecting the occipital and parietal bones and sagital suture were connecting the parietal bones close in the 30s. He thought that these findings explain the development of hyperpneumatization extending into the occipital bone and from it through the lambdoid and sagital suture into the parietal bone. The whole process takes at least 3 decades to reach a maximum stage, leaving only thin tabula interna and external.
There has been a description of variable scutum anatomy such as the scutum “pseudotumor” appearance caused by incomplete pneumatization was seen frequently, and should not be mistaken for mastoiditis or an osteoma [4]. However, to the best of my knowledge, there has been no report of elongated scutum presenting as a white mass behind an intact tympanic membrane.
This report will highlight the importance of retaining a wide differential diagnosis in the workup of a middle ear mass like lesion behind an intact tympanic membrane.
Conflict of Interest
None.
Role of the Funding Source
None.
| References | ▴Top |
- Semaan MT & Fayad JN (2008) White mass in the middle ear. Ear, nose, & throat journal 87(11):610-611.
pubmed - Rebol J, Munda A, & Tos M (2004) Hyperpneumatization of the temporal, occipital and parietal bones. Eur Arch Otorhinolaryngol 261(8):445-448.
doi pubmed - Madeline LA & Elster AD (1995) Suture closure in the human chondrocranium: CT assessment. Radiology 196(3):747-756.
pubmed - Virapongse C, Sarwar M, Bhimani S, Sasaki C, & Shapiro R (1985) Computed tomography of temporal bone pneumatization: 1. Normal pattern and morphology. AJR. American journal of roentgenology 145(3):473-481.
pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Cases is published by Elmer Press Inc.